Establishing Clinical Normative Data for Wideband Tympanometry Measurements

Abstract
In recent years, researchers have found evidence that Wideband Acoustic Immittance (WAI) measurements, specifically Wideband Tympanometry (WBT), to be more sensitive than conventional single frequency immittance testing at differentiating normal ears from pathological ears. However, normative data, obtained primarily from research instrumentations, have been shown to be greatly affected by ethnicity, gender, and age. For WBT to be more widely implemented in clinical settings, normative data that are collected from specific clinical populations and obtained by commercially available clinical instrumentation are needed. The primary goal of this study is to establish WBT normative data for the population served at University of the Pacific Hearing and Balance Center in San Francisco, US.
Introduction
As a clinically diagnostic test, it is essential that tympanometry is both sensitive and specific to middle ear conditions. Studies in children populations with otitis media with effusion (OME) revealed that tympanometry using a 226 Hz probe-tone was generally accurate.1 On the other hand, the test was unable to distinguish normal ears from otosclerotic ears.2 Other researchers have concluded that 226 Hz probe-tone tympanometry is insensitive to otosclerosis and ossicular chain discontinuity.3 In fact, one study measured the compliance of 34 confirmed individuals with otosclerosis and compared it with 34 randomly chosen normal hearing individuals (controlled for age and gender). The results showed a large overlap of the values obtained. This may translate to a large number of false negatives of the otosclerotic population or a large number of false positives of the normal hearing population.4 Naturally, alternative testing of the middle ear system, including WBT, has since been explored.
It is also important to consider age and gender differences in the measurements of Equivalent ear Canal Volume (ECV), Peak Static Admittance, and Tympanometric Peak Pressure (TPP). Research has found that there are differences between ethnicities. For example, Chinese individuals generally had smaller admittance values, a more positive TPP, larger TW values, and smaller ECV values.2 Thus, when establishing normative values, these variables must be taken into consideration.
The goal of this study is to collect and establish WBT normative data for population served at University of the Pacific (UOP) Hearing and Balance Center, using commercially available equipment. Results from this study could build a foundation where clinicians at our clinic could start to implement WBT measurements in the routine audiological assessment protocol, using our own clinical equipment. With more data and further investigation, it could help clinicians examine and diagnose middle ear pathology, such as otosclerosis, more effectively.
Methods
All testing was conducted in San Francisco at University of the Pacific (UOP) Hearing and Balance Center. This study is approved by the Institution Review Board at UOP. Thirty-five subjects were recruited from the doctor of audiology program and consisted of students and faculty members. The range of ethnicities of the participants is representative of the patient population served by our clinic. All subjects underwent a routine audiological assessment prior to the WBT data collection to insure normal hearing sensitivity and no middle ear pathology. A Madsen Astera 2 audiometer (GN Otometrics, Taastrup, Denmark) and a Titan 3.1 (IMP440, Denmark) tympanometer was used to perform audiometry and traditional 226-Hz single frequency tympanometry. For WBT data collection, we used the same Interacoustics Titan 3.1 equipment. A broadband (226 Hz to 8000 Hz) click was used as the probe tone.
Conventional 226 Hz tympanometric data and WBT measurements were collected from each subject. WBT measurements included power absorbance, resonance frequency (RF) of the middle ear, and other tympanogram data. Power absorbance represents the amount of energy absorbed by the middle ear. RF measured is the RF of the middle ear and is detected at middle ear pressure.
Results
Power Absorbance
The distribution of power absorbance values across frequencies were illustrated in Figure 1.
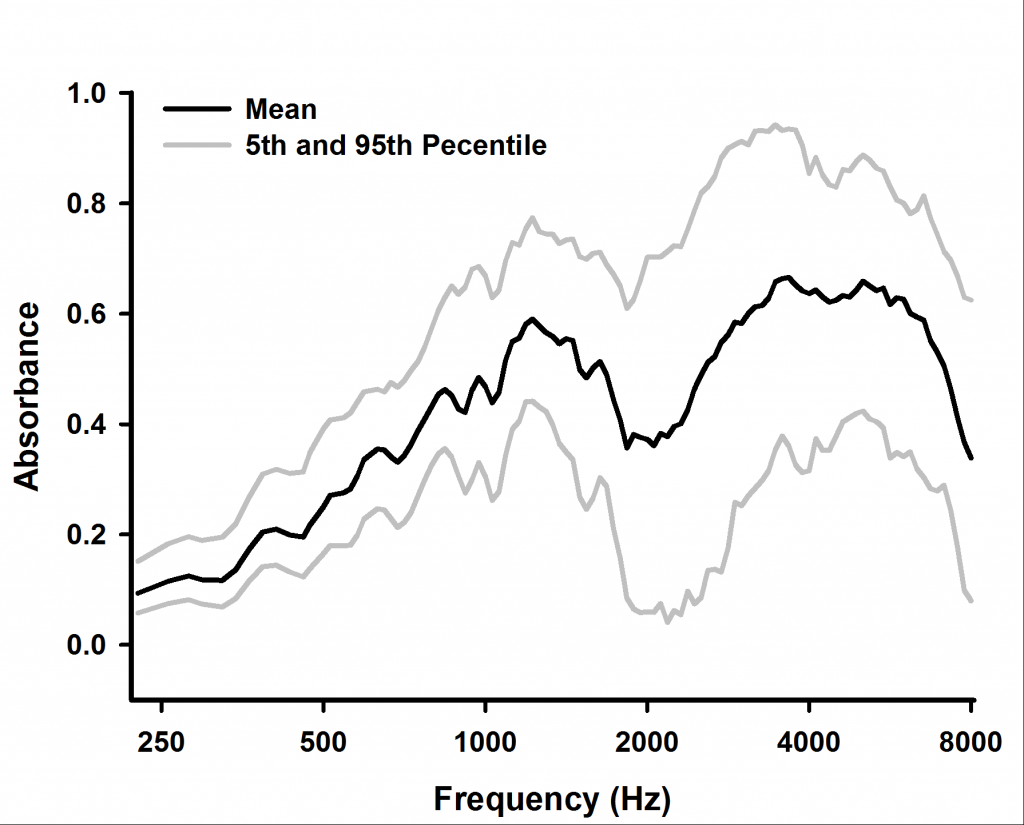
Figure 1. Distribution of absorbance across frequencies.
An example of using this normative data is shown in Figure 2. Subject 20, whose data was not included in the normative data set, was born without a stapes in her left ear. When the same WBT protocol was applied in her measurement, her absorbance measurement was plotted against the normative data.
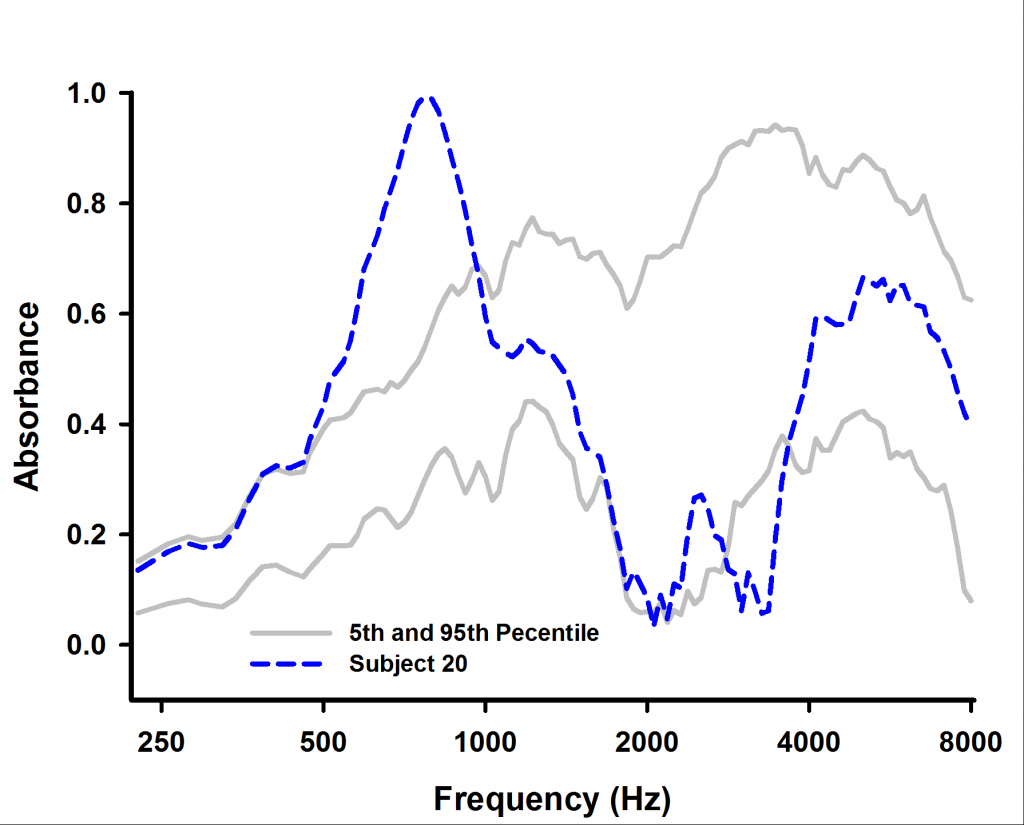
Figure 2. Power absorbance of a patient with missing stapes in one ear.
Conventional and Derived Single Frequency Tympanometry (SFT)
One of the features included in the Titan’s WBT measurements is that the system can derive tympanograms at different probe frequencies based on the broadband stimulus. For example, it provides a 226-Hz tympanogram that is extracted from the WBT. We compared the admittance that were obtained from both conventional SFT and derived SFT. Figure 3 demonstrates the result of such comparison.
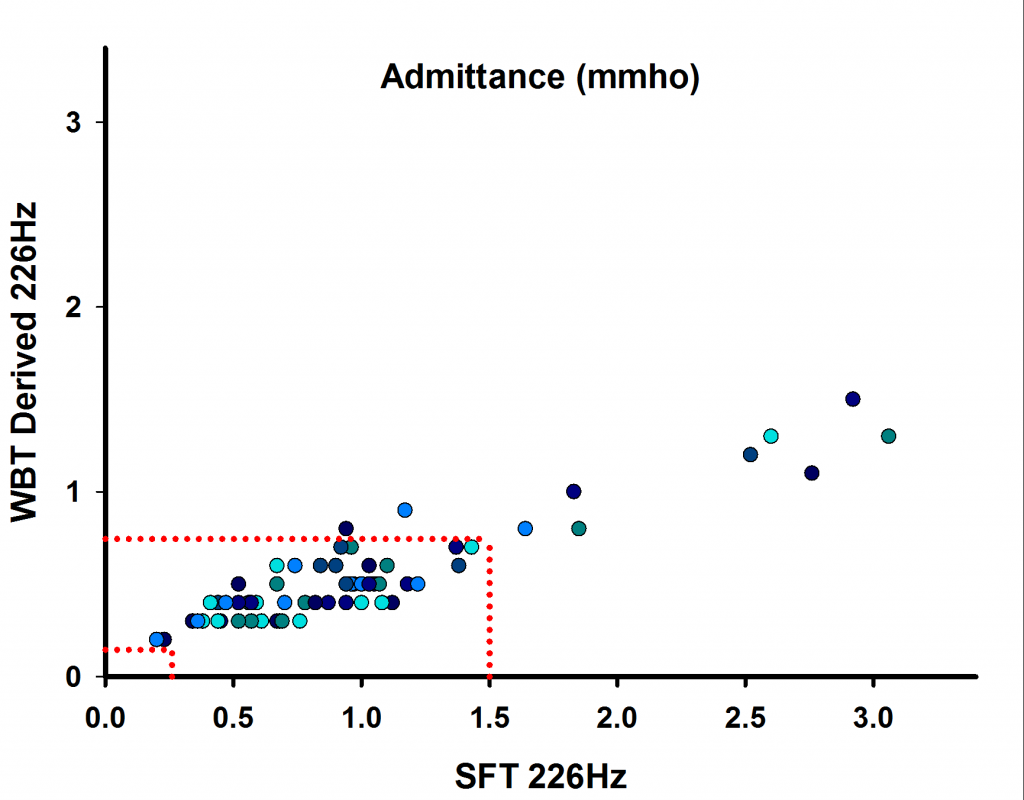
Figure 3. Comparison of admittance values that were obtained from conventional SFT and derived from WBT. Dotted red lines represent the normative range of conventional SFT admittance used by our clinic.
A simple linear regression analysis was performed on admittance values obtained from conventional and derived SFT (R = 0.914, p < 0.001). The normative range of conventional SFT admittance used by our clinic is 0.3–1.5 mmhos. Based on this range and the regression result, we calculated the normative range of admittance values (0.145–0.745 mmhos), for the use of 226 Hz tympanometry that is derived from WBT measurement.
Comparison of SFT and Derived: ECV and TPP
Similar to the admittance values, Equivalent Canal Volume (ECV) and Tympanometric Peak Pressures (TPP) measurements with 226 Hz probe tone can also be derived by the WBT system. We compared the ECV and TPP values that were obtained from both conventional SFT and derived SFT. Figure 4 and Figure 5 demonstrate the result of such comparisons. Figure 4. Comparison of ECV values that were obtained from conventional SFT and derived from WBT.
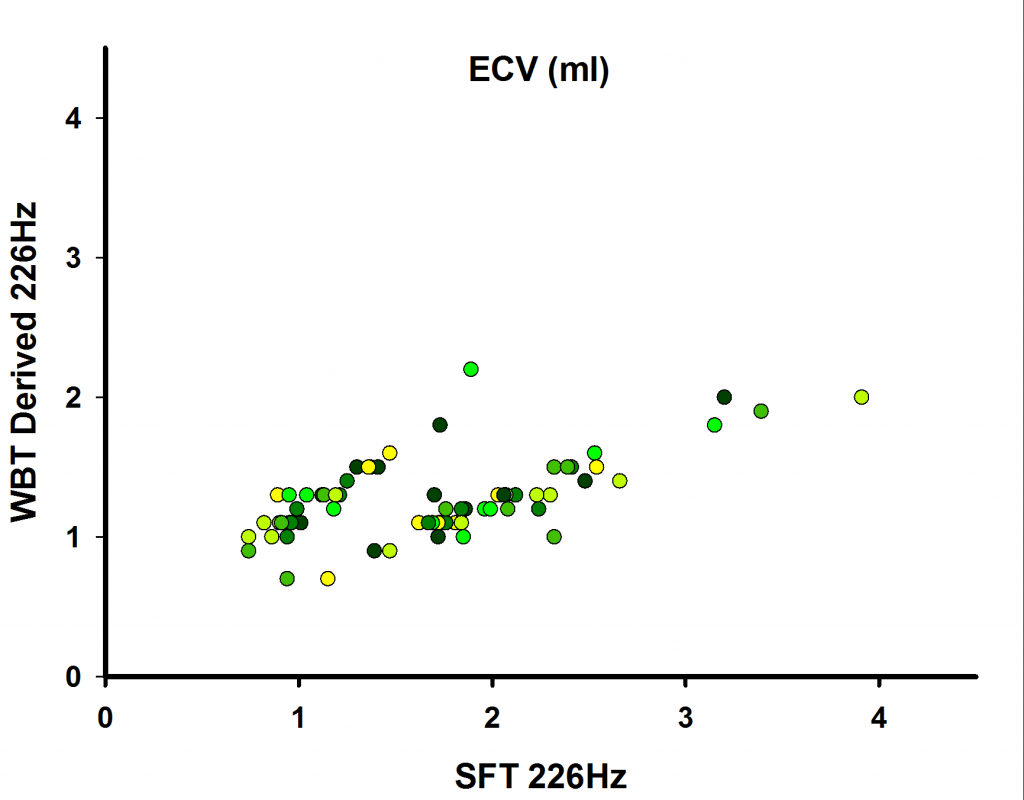
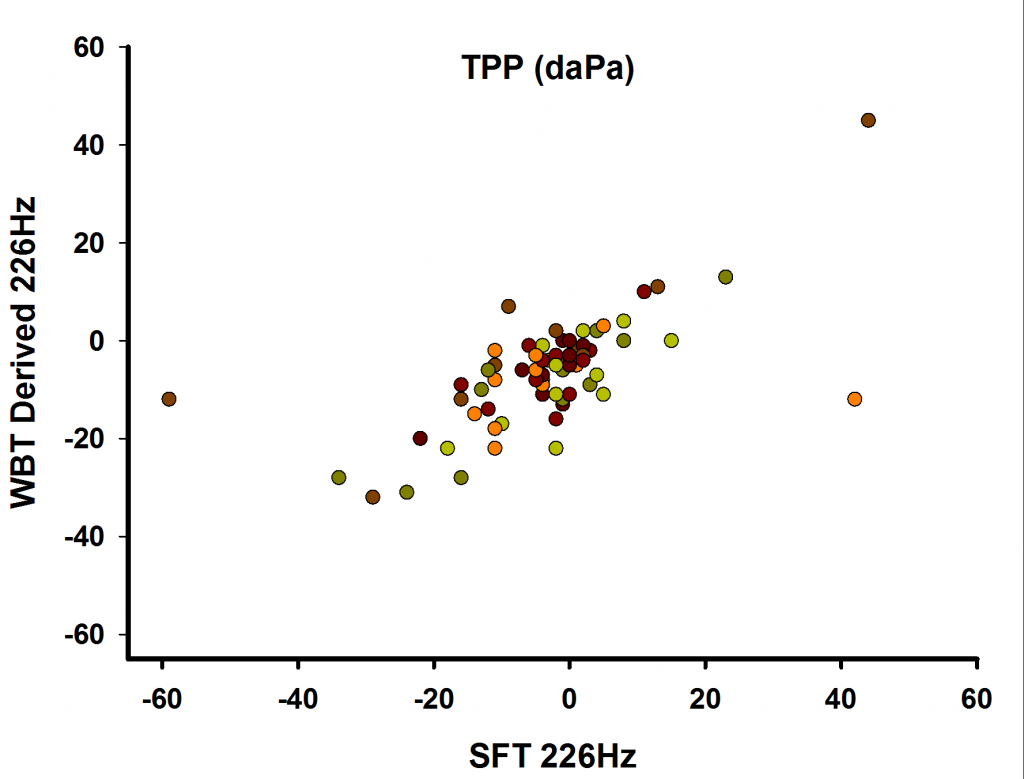
Figure 5: Comparison of TPP values that were obtained from conventional SFT and derived from WBT.
Simple linear regression analysis were performed on ECV and TPP values obtained from conventional and derived SFT (R = 0.608, p < 0.001, and R = 0.663, p < 0.001, respectively).
Resonance Frequency of the Middle Ear
RF of the middle ear, which is not available in SFT, is an index that has been shown to be clinically relevant. Figure 6 illustrates the comparison between the admittance values that were obtained from conventional 226 Hz SFT and RFs that were obtained from WBT at ambient pressure.
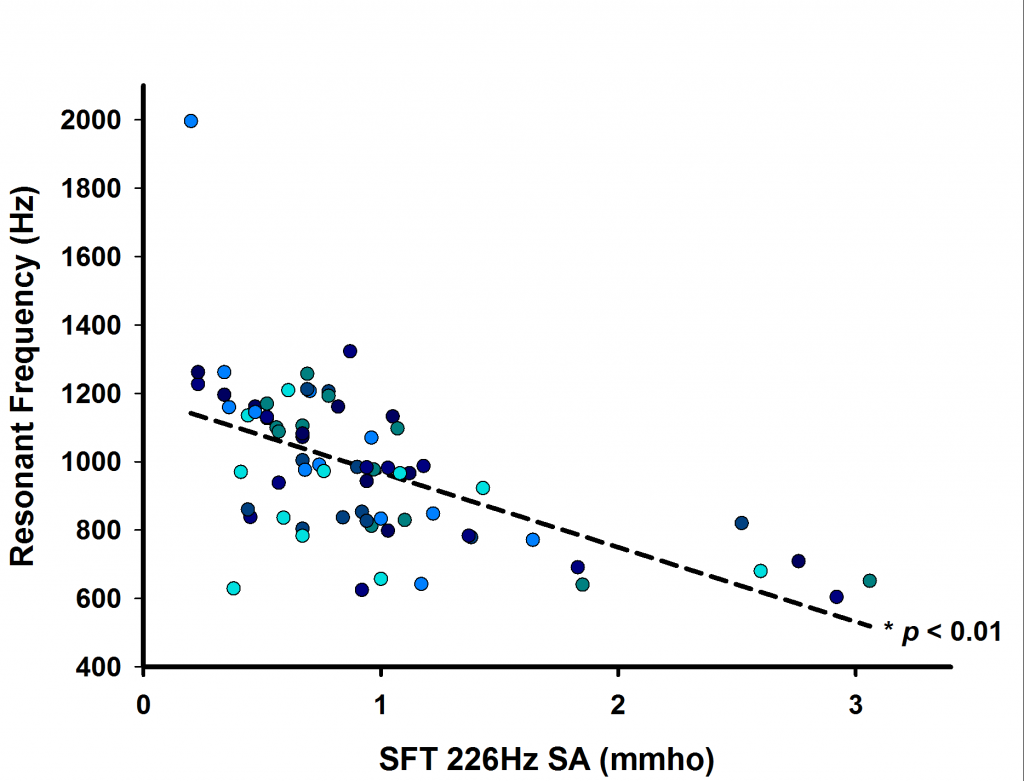
Figure 6: Linear regression between admittance values of conventional 226 Hz SFT and Resonance Frequencies (RF) that were obtained from WBT.
A statistically significantly correlation (p > 0.01) was found between the two indexes, which is not surprising given that they depend on the same physical properties of the middle ear system, such as stiffness and mass, etc.
Discussion and Conclusion
Results from this study demonstrated the efficacy of implementing WBT into a typical audiological assessment protocol, and some factors to consider for such implementation. For example, the new normative admittance range, illustrated in Figure 3, suggests that if one plans to incorporate WBT clinically and use the 226 Hz tympanometry results that are derived from WBT instead of using conventional stand-alone SFT, the clinician must take caution of using any existing clinical norms that were used for conventional SFT and must establish their own norms, using similar techniques like we did. The correlation between RF of the middle ear and conventional tympanometry’s admittance is also very interesting that, as suggested,2 with further investigation into RF, it may prove itself to be a viable clinical assessment tool in the future.
We plan to expand our study to have more normative data points and to include data collection sites with different ethnic patient populations. With further investigation on WBT, it could potentially help clinicians examine and diagnose middle ear pathologies, such as otosclerosis, more effectively.
References
- Shahnaz N, Bork K, Polka L, et al. Energy reflectance and tympanometry in normal and otosclerotic ears. Ear Hear 2009;30(2):219–33.
- Hunter LH and Shahnaz N. Wideband reflectance principles. Acoustic immittance measures. San Diego: Plural Publishing; 2014.
- Feeney MP, Grant IL, and Marryott LP. Wideband energy reflectance measurements in adults with middle-ear disorders. J Speech Lang Hear Res 2003;46:901–11.
- Browning GG, Swan L, and Gatehouse S. The doubtful value of tympanometry in the diagnosis of otosclerosis. J Laryngol Otol 1985;99(6):545–47.
- Iacovou E, Vlastarakos PV, Ferekidis E, Nikolopoulos TP. Multi-frequency tympanometry: clinical applications for the assessment of the middle ear status. Indian J Otolaryngol Head Neck Surg 2013;65: 283–87.