From the Labs to the Clinics

From the Labs to the Clinics
Renowned auditory researcher Dr. Robert Harrison brings us up to date on information and research from the Labs. Appropriately titled “From the Labs to the Clinics”, Bob is involved in laboratory and applied/clinical research, including evoked potential and otoacoustic emission studies and behavioural studies of speech and language development in children with cochlear implants. For a little insight into Bob’s interests outside the lab and the clinic, we invite you to climb aboard Bob’s Garden Railway.
In Praise of Noise Dosimetry
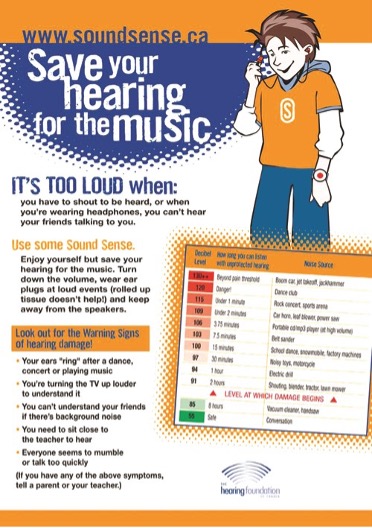
We have seen much “new knowledge” that can potentially impact hearing healthcare. For example, haircell growth from stem-cells, auditory nerve regeneration, gene therapy, the role of AI in hearing prosthesis development and employment, etc. I have covered some of these areas in previous “Labs to Clinics” columns. Most of these new developments relate to possible hearing restoration. Today, however, rather than discuss possible new ways to treat hearing loss, I want to revisit some existing concepts and methods in audiology for the prevention of noise-induced hearing loss. For many years I was involved in the prevention of noise-induced hearing loss in children, particularly education campaigns about the safe use of personal sound entertainment devices, originally cassette and MP3 players, more recently smartphones and videogame devices. See Figure 1 below [1, 2]. For the most part, we are (I hope) much more aware about the risks of exposure to loud acoustic signals.
In the broader field of environmental and occupational noise, I have come to appreciate the role of Occupational Health and Safety (OHS) specialists (often together with Audiologists) and their methods of noise dosimetry. The basic concepts of noise exposure dosimetry are not new, having been established soon after the Second World War. This methodology has been most instrumental in limiting harmful noise exposure and establishing safe working conditions (often backed by legislative guidelines). Noise dosimetry deserves some good press!
We all understand that acoustic trauma is not the same as noise-induced hearing loss (NIHL), although I have often seen the terms used interchangeably. Perhaps there are some formal definitions, but for me it is simple. If an acoustic signal is at a pressure level that can physically injure the ear(s), and cause an immediate and permanent hearing problem, then it is acoustic trauma. At the less severe end of the scale, a much lower-intensity noise exposure over long periods can lead to hearing problems. This is how I would characterize noise-induced hearing loss. Here, the hearing loss risk depends on both signal intensity and duration. A relatively intense, 30-second acoustic signal can have the same risk as 8 hours of continuous low-level noise.
If you are in an environment where the noise level feels excessive, it is routine to consult the sound level app on your phone (no self-respecting audiologist is without the app). The revealed level may be uncomfortable (as in “let’s get out of this restaurant”), but it will not definitively indicate risk of NIHL without an exposure duration. The intensity/time trade-off is the key feature about noise dosimetry.
Noise exposure dosimetry involves continuous monitoring of acoustic signal levels (usually A-weighted) using a microphone attached to the body, typically at shoulder level, together with a data storage device. In the occupational health and safety world, this monitoring is often conducted over a full working shift or a long-term period in a representative sound environment. Most often the goal is to measure a long-term average exposure level over an 8-hour workday (in any 24-hour period). Based on hundreds of published studies, the daily noise dose that can pose a risk of hearing loss has been established and formally adopted by health and safety regulatory bodies. For example, we have the Canadian Centre for Occupational Health and Safety (CCOHS) [4] the Occupational Safety and Health Administration (OSHA) in the US [3]. There are multiple jurisdictions worldwide, but all have set similar guidelines about the length of time that a person can be exposed to various levels of continuous noise before there is a risk to hearing. This is set at 85-87 dBA for an 8-hour time-weighted average (TWA) over any 24-hour period. This level is referred to as an action level at which some mitigation procedure must be implemented, often requiring the mandatory use of hearing protectors. In Canada this risk threshold (action level) is set at 87 dBA TWA.
Table 1 below is based on Canadian Centre for Occupational Health and Safety guidelines [ref 4] and shows the relationship between noise exposure level and permissible exposure time. I have indicated on this table the relevant risk threshold of 87 dBA for an 8hr daily exposure.
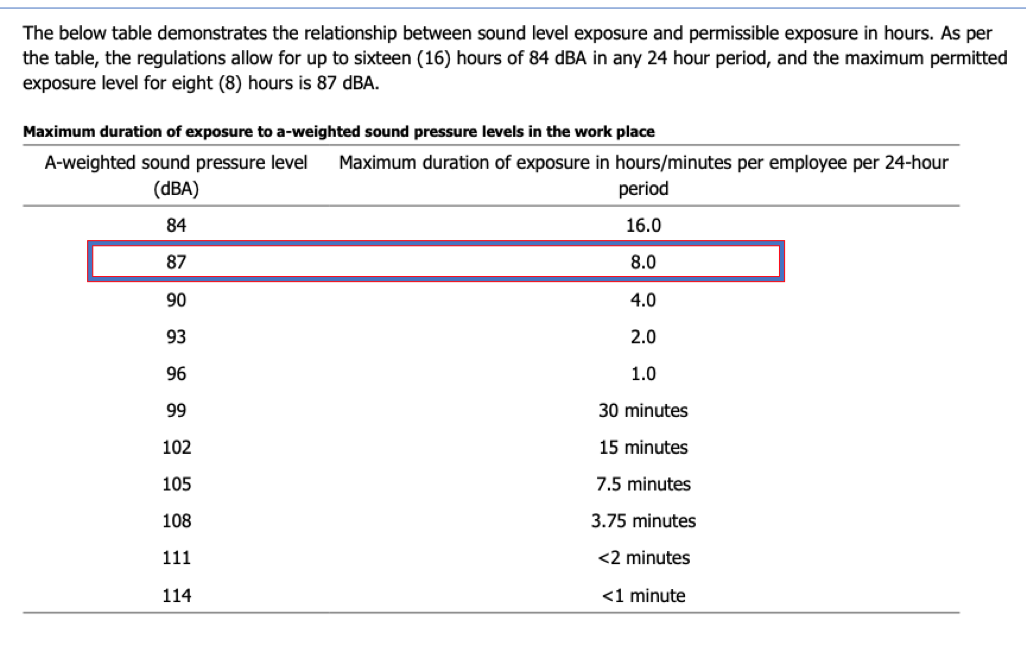
To reiterate, the important concept in dosimetry is the trade-off between noise exposure level and duration. Table 1 shows a range of long-term average noise levels (left column) versus exposure duration (right) that can pose a risk of noise-induced hearing loss. The table is a useful reference guide to many more noise exposure situations than just the occupational “working day”. The table indicates the risk thresholds for noise exposure across various signal intensities and durations.
Indeed, there are numerous useful applications of noise dosimetry beyond the formal workplace. There are dosimetry studies of road traffic noise, train and airport noise, construction-site noise, entertainment venue music levels, and crowd noise. One study I have been involved in has evaluated the health effects of exposure to wind-turbine noise [5].
In legal liability issues and in workers' compensation board decisions, noise dosimetry is an essential tool in evidence.
I offer my appreciation to the occupational health and safety pioneers for developing a practical approach to hearing-loss risk assessment. These schemes have likely prevented more noise-induced hearing loss than any other policy.
References
- HARRISON RV. (2008). Noise-induced hearing loss in children: A ‘less than silent’ environmental danger, Paediatrics & Child Health, Volume 13, Issue 5, May/June 2008, 377–382. https://doi.org/10.1093/pch/13.5.377
- HARRISON RV. (2012) The prevention of noise induced hearing loss in children. International Journal Pediatrics, 2012 Article ID 473541, pp13 doi: 10.1155/2012/473541 https://doi.org/10.1155/2012/473541
- Occupational Safety and Health Administration (OHSA). Noise exposure standards https://www.osha.gov/noise/standards
- Canadian Centre for Occupational Health and Safety (2025). Noise, occupational Exposure limits in Canada. https://www.ccohs.ca/oshanswers/phys_agents/noise/exposure_can.html
- Understanding the Evidence: Wind Turbine Noise. Ottawa: The Expert Panel on Wind Turbine Noise and Human Health, Council of Canadian Academies. ISBN 978-1-926522-07-4