The Auditory Brainstem Response: Still an Important Tool for Neurodiagnostics!

The auditory brainstem response (ABR) in humans was first reported by Jewitt and colleagues in 1970,1 with reports of assessing brainstem integrity following shortly afterwards. It has since become one of the most utilized diagnostic tests in the audiologist’s test battery, providing a functional assessment of the eighth nerve, pons and more caudal portions of the auditory system. The response reflects the synchronous discharge of auditory neurons along the eighth nerve and brainstem structures occurring within 10 msec after auditory stimulation, as measured at the scalp. The primary generators of the waves are thought to be as follows: wave I – distal portion of eighth nerve, wave II – medial portion of eighth nerve, wave III – cochlear nucleus, wave IV – fibers from the superior olivary complex, and wave V – lateral leminiscus termination in the contralateral inferior colliculus, although there are multiple generators sites for waves III and beyond.2 Latency measurements are typically made for the three major waves: I, III and V. Diagnostically, the absolute, interpeak and interaural latencies are measured and compared to age-appropriate normative data and yield high sensitivity in detecting lesions along the auditory pathway.2 Amplitude measurements of wave V/I have proven useful in assisting detection of certain conditions.3 Increased in stimulation rates and changes in stimulus intensity can also help detect brainstem lesions.4
One of the most exciting findings for the ABR was that it could be used to detect vestibular schwannomas.5 These tumours generally arise from the vestibular portion of the eighth nerve but because they generally cause a hearing loss, the term “acoustic” tumours is commonly used. Many early studies reported detection rates between 93 and 100%,6 but detection rates were poorer for small tumours (< 1 cm) that could nonetheless be easily identified by magnetic resonance imaging (MRI). For example, Cueva7 found abnormal ABRs in only 22 out of 31 patients with vestibular schwannomas and other hearing-related tumours, but 7 of the 9 patients with normal ABRs had small tumours (identified via MRI). For this reason, the MRI has become the standard in detecting vestibular schwannomas and the use of the ABR for this purpose has been discouraged. However, a recent meta-analysis6 suggests that the ABR should not be abandoned in favour of MRI. Across 43 studies which met the inclusion criteria for the analysis (involving 3,314 patients), the pooled sensitivity of the ABR was 95.6% for tumours greater than 1 cm and 85.8% for tumours less than 1 cm, with an average pooled sensitivity of 93.4%. Given these high detection rates, the authors strongly urge a reconsideration of the ABR as a useful diagnostic tool, particularly in light of the trend toward more conservative management of vestibular schwannoma, and the expense associated with MRI-based testing. Direct MRI referral protocols based on audiometric screening criteria (i.e., interaural asymmetries) that have reasonable levels of sensitivity – greater than 90% – have specificities below 45%,8 whereas the average pooled specificity of neurodiagnostic ABR, based on 8 studies that met inclusion criteria (2,432 patients), is 82.0%.6 Moreover, although many large centres have MRI available, rural medical settings may not have access to such technology or the medical specialists, and the ABR can play an important role in such cases, at least for initial investigations.
Audiologists and the medical community should also be reminded that ABR is an important tool for assessing suspected diseases of the brainstem up to the level of the pons. There are over 50 disorders that have been reviewed in the scientific literature that can affect the pediatric and adult brainstem9 and there are disorders that have an impact on the ABR but not upon the structural MRI.10 Moreover, unlike the MRI, the ABR provides detailed information about the functional capabilities of the auditory brainstem.
The following case example provides support for ABR inclusion in diagnostic protocol. A five-year-old girl was seen in the clinic with complaints of concern for speech and language development. The child had previously passed newborn hearing screening. Parental report noted she often misunderstood auditory information, never heard song lyrics correctly and was extremely sensitive to any background noise. The remainder of the medical history was negative. Objective measures revealed normal middle ear status bilaterally but elevated contralateral acoustic reflexes. Distortion product otoacoustic emissions were normal bilaterally from 1000 to 8000 Hz in both ears. In the booth, the child appeared reluctant to respond to both pure tones and speech stimuli. Out of concern for the abnormal acoustic reflex pattern, the audiologist performed a diagnostic ABR. Click stimuli were presented at 80 dB nHL to each ear using insert phones. The left ABR was normal for all measures. The right ABR’s traditional measures were normal. However the audiologist noticed that wave IV on the right side was not replicating and appeared dysmorphic in comparison to the other waves, while the wave V for the right was slightly earlier (see Figure 1). Medical consultation gave rise to a neurology consultation. MRI revealed that the child had a type I (mild) Arnold Chiari malformation on the right side. This condition occurs when the brain tissue is forced through the opening at the base of the skull. The child is now followed up regularly and as of yet there has been no determination regarding surgical treatment.
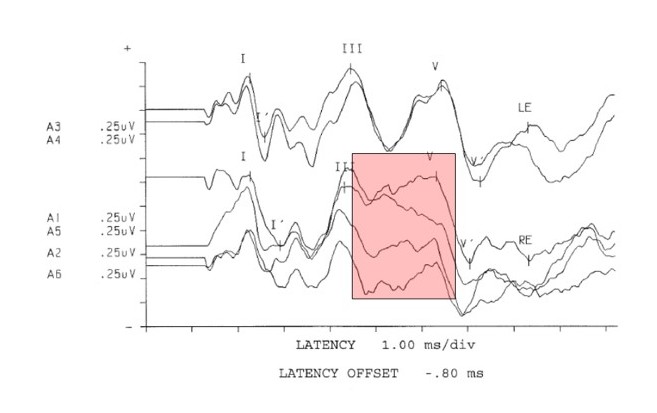
Figure 1. Neurodignostic click (80 db nHL) auditory brainstem response from a five-year-old girl with auditory complaints. Note the area highlighted revealing difficulty replicating wave IV and a slightly early wave V on the right. All measures were within normal values compared to normative data for 5 year olds.
While the MRI is the gold standard for the detection of vestibular schwannomas, it is important for our profession to recognize the importance and value of the ABR for clients of all ages. The ABR may serve an important diagnostic role when MRI is not readily available or as part of a detection protocol, and it provides valuable functional information not provided by MRI. There are many disorders that can impact the brainstem. When audiological “red flags” appear, such as abnormal acoustic reflex patterns and disproportionate auditory complaints, as in the presented case, it is the audiologist’s duty to perform further neuroaudiological testing.
Our profession should be doing more to foster inter-professional collaboration within the medical community. Electrophysiological testing can be helpful in this regard – not only for screening and diagnostics – but also for providing useful functional data for disease monitoring and outcome measures following treatment. In the end, we are all working towards a common goal for our clients.
References
- Jewett DL, Romano MN, Williston JS. Human auditory evoked potentials: Possible brainstem components detected on the scalp. Science 1970;167:1517–18.
- Moller AR. Hearing: Anatomy, Physiology and Disorders of the Auditory System, 3rd edition. San Diego: Plural Publishing; 2013.
- Musiek FE, Lee WW. The auditory brain stem response in patients with brain stem or cochlear pathology. Ear Hear 1995;16:631–6.
- Bush ML, Jones RO, Shinn JB. Auditory brainstem response threshold difference in patients with vestibular schwannomas: a new diagnostic index. Ear Nose Throat J 2008;87:458–62.
- Selters W, Brackmann D. Acoustic tumor detection with brain stem electric response audiometry. Arch Otolaryngol 1977;103:181–7.
- Koors PD, Thacker LR, Coelho DH. ABR in the diagnosis of vestibular schwannomas: a meta-analysis. Am J Otolaryngol 2013;34:195–204.
- Cueva RA. Auditory brainstem response versus magnetic resonance imaging for the evaluation of asymmetric senorineural hearing loss. Laryngoscope 2004;114:1686–92.
- Cheng TC, Wareing MJ. Three year ear, nose and throat cross-sectional analysis of audiometric protocols for magnetic resonance imaging screening of acoustic tumors. Otolaryngol Head Neck Surg 2012;146:433–47.
- Hall JW. New Handbook of Auditory Evoked Potentials, 1st Ed. Pearson; 2006.
- Peterein JL, Neely JG. Auditory brainstem response testing in neurodiagnosis; structure versus function. J Am Acad Audiol 2012;23:269–75.