Considerations in Real-Ear Measurement: Points to Ponder

Verification via real-ear measurement (REM) is an important part of the hearing instrument provision process should the benefits of amplification be fully realized. It has been well established in the literature that hearing instruments often do not deliver what is anticipated relative to fitting formula targets upon quick fit,1,2 that the device output on hearing instrument fitting software does not always convey what is actually being delivered by a device in the ear canal3,4 and that these differences can be large and significant on the order of +/- 10 dB or more.5 While debate sometimes arises regarding the appropriate prescriptive target to use for a particular fitting, it is generally established that the use of a validated generic fitting formula is a good place to start. Multiple research studies have now documented the benefits to be achieved in hearing outcomes for patients wearing a verified hearing aid adjusted to fitting formula targets versus unverified quick fits, both in lab-based and real-world environments.6–8
It is at least partially for these reasons that numerous professional bodies have indicated in their preferred practice guidelines that verification (i.e., REM) should be performed during the fitting of hearing instruments. Unfortunately, what is recommended in practice does not always make it to the clinic, and multiple surveys over the years9,10 have indicated roughly only 35–55% of clinicians routinely conduct probe microphone testing / REM during the fitting of hearing aids. Numerous reasons have been proposed for the lack of use of verification, including perceived lack of benefit, the amount of time involved and the perceived complexity of the procedure just to name a few. While there may have been a time where some of these objections were valid, we now have much evidence which shows otherwise and improved REM instrumentation which makes these procedures easier than ever before.
For those clinicians who do conduct REM, questions sometimes arise regarding proper techniques and measurement considerations - to ensure the greatest likelihood of measurement accuracy and increase the probability that any associated conclusions are indeed valid. Given the popularity of “open fit” devices, it is likely not too surprising that many of these questions often relate to this product type. Understandably many of these concerns reference the ‘unique’ acoustic realities of this type of product fitting versus more occluded hearing instrument types. In particular, the concept of acoustic transparency and any associated impact on the fitting procedure is often referenced, given the relatively smaller impact of an open fit product on the patient’s ear canal resonance. Furthermore, the need for considerations regarding the combination of direct (i.e., vent-transmitted sound) and indirect (i.e., amplified sound) provided by the hearing instrument leads many to wonder, what if anything they should adjust in their verification protocol. It is with these thoughts in mind that this article will attempt to highlight some verification considerations unique to open fit products and how they might impact decision-making during the hearing instrument fitting process.
Historically, there have been 2 primary camps for target matching with REM – the relatively older “real-ear insertion gain” (REIG) approach and the more recent “real-ear aided response” approach (REAR) – used with the SPL-o-gram method popularized in large part by the Desired Sensation Level (DSL) group (see Table 1 for some relevant REM definitions). While arguably the majority of audiologists now use the REAR for verification, some prefer to use the REIG method, likely due to familiarity with this technique over the relatively more recent REAR / SPL-o-gram approach.
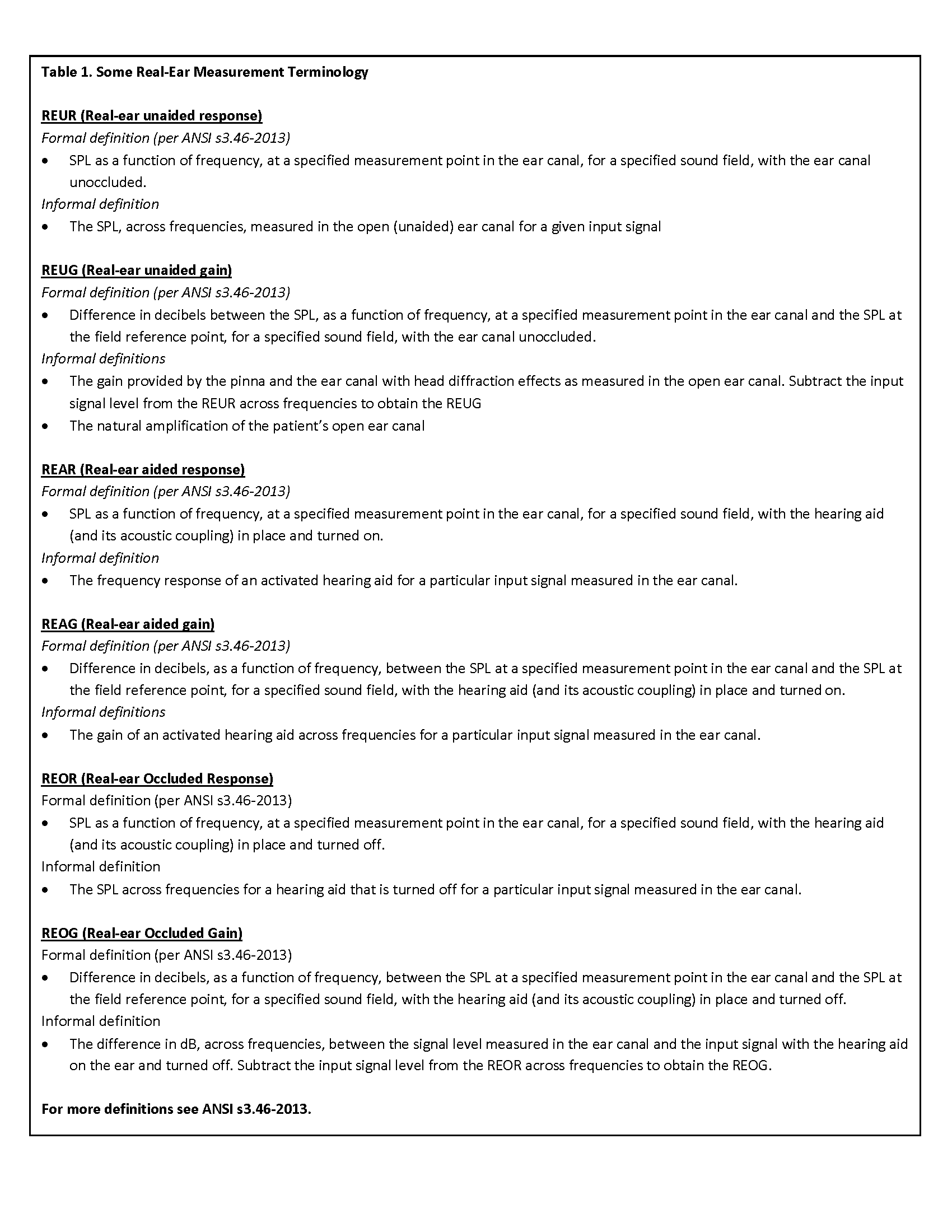
By way of a brief review, real-ear insertion gain (REIG) was developed as an electroacoustic equivalent to functional gain11 which represented the differences between unaided and aided thresholds in sound field across frequencies. The real-ear unaided response (the SPL across frequencies measured in the open (unaided) ear canal for a given input signal) was deemed to capture the unaided audiogram while the real-ear aided response (the SPL across frequencies measured in the aided ear canal) was deemed to capture the aided audiogram. Real-ear insertion gain was then simply represented as the REAR – REUR as shown in Figure 1.
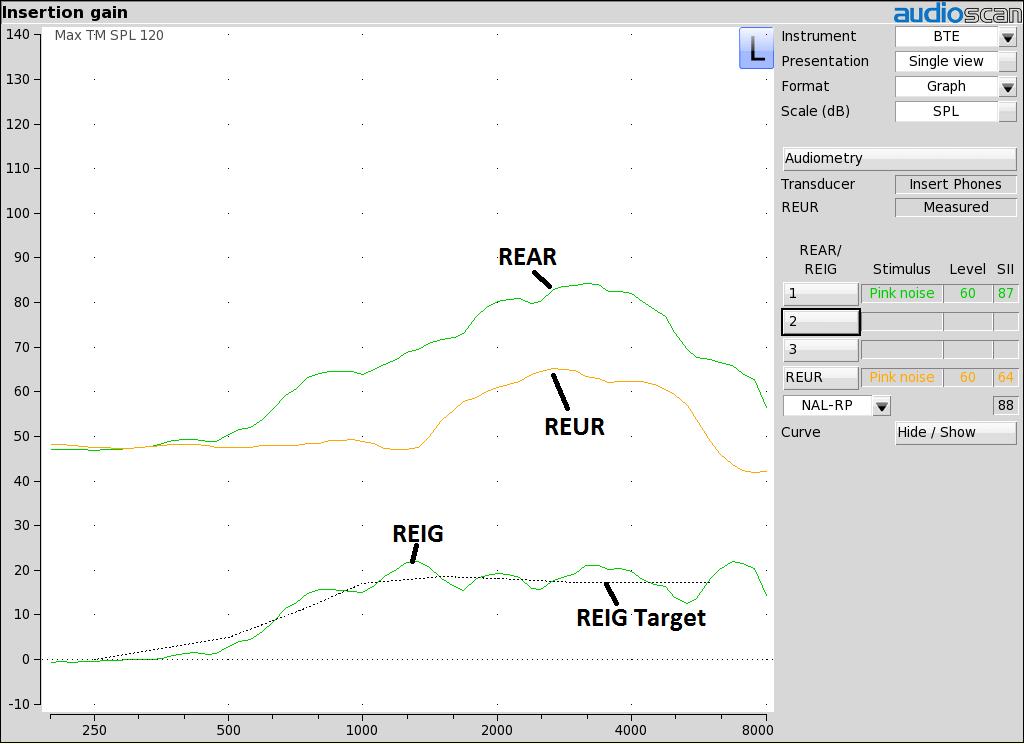
Figure 1. Example of a real-ear aided response (REAR) measurement, obtained with a 60 dB SPL pink noise signal. Also shown is the previously measured real-ear unaided response (REUR) measurement, along with the resulting real-ear insertion gain (REIG) values and the REIG target.
The REIG approach does present with some limitations relative to the SPL-o-gram (REAR only) method, including the absence of a frame of reference regarding the impact of target mismatches on audibility and/or implications relative to a patient’s uncomfortable loudness levels (i.e., lack of dynamic range visibility). In addition, insertion gain approaches inherently assume a sound field audiogram given their inclusion of the open ear (i.e., REUG) in their target calculation. Needless to say, sound field audiograms are rarely if ever conducted with adult patients, let alone with pediatric patients, given the need for ear-specific audiometric data, thus arguably limiting the usefulness of including the REUG in any prescriptive approach. Furthermore, as the REIG calculation approach is influenced by the individual nature of the patient’s REUR/REUG (see Figure 2), unusual REURs/REUGs containing valleys or dips in the high frequencies can impact the perceived suitability of a hearing aid fitting relative to target – not to mention the ability in some cases to achieve the target in question. It is for this reason that you sometimes run across the old adage – if you want to hit your REIG target – find someone with a small REUG; an aspect that isn’t entirely logical, particularly if the REUG was not part of the assessment (i.e., testing was not conducted in sound field) and the patient has the same hearing loss (or more specifically the same dB SPL at the eardrum requirements for audibility) as someone else with a larger REUG. Understandably some question why the required SPL level at the eardrum to achieve desired performance should differ in the example described above. This conundrum has led many to advocate for using an average REUG in the calculation12 and/or to leverage the significant relative benefits of the REAR approach as will be touched on below.
Questions related to the appropriate REUG to consider in the verification process has similarly led some REM systems to recommend using only average REUG values for REIG calculation unless the audiometric assessment was performed in the sound field. Specifically, it has been advised that measured REURs should only be used when thresholds were obtained in sound field as the individual REUR was then part of the assessment and therefore should be considered in target calculation. In all other cases, the average REUR provided by the fitting formula developers should be used because the individual REUR was not involved in the assessment.
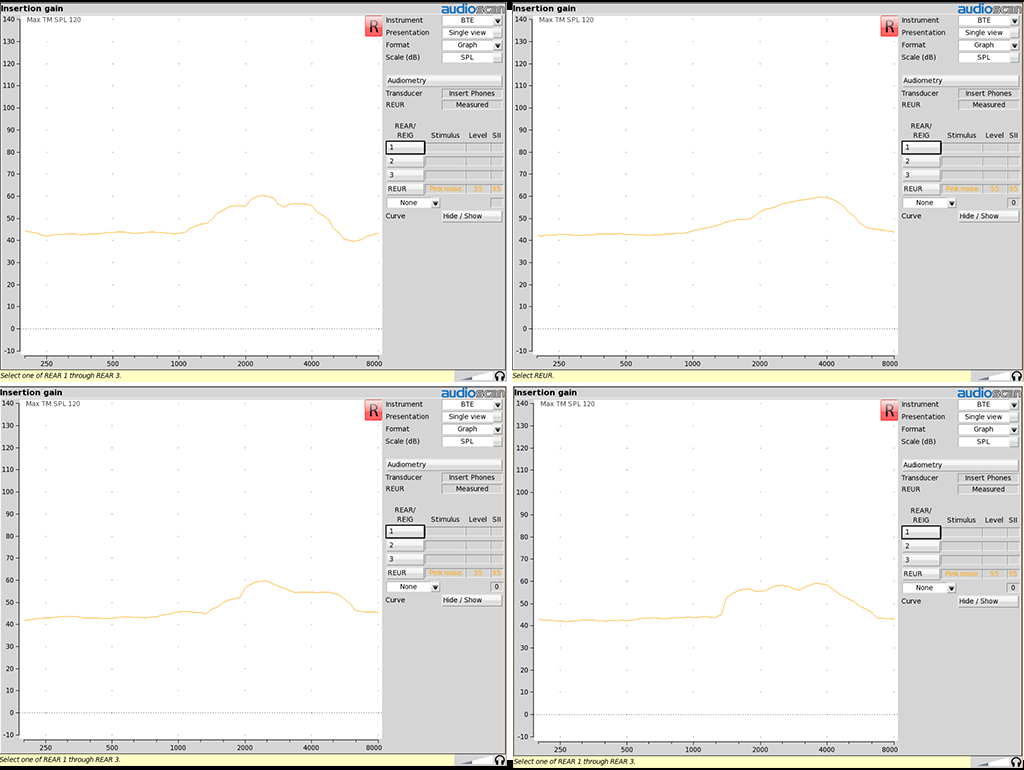
In contrast to the REIG approach outlined above and shown in Figure 1, the REAR method provides an indication of the relationship of all relevant variables at all points in the fitting (see Figure 3) – for example, the impact of a missed target on audibility. We also now have an indication of the dynamic range of the patient and can quickly assess not only the audibility of a particular signal, but also the relationship of the hearing instrument output relative to the measured (or predicted) uncomfortable listening levels of the patient.
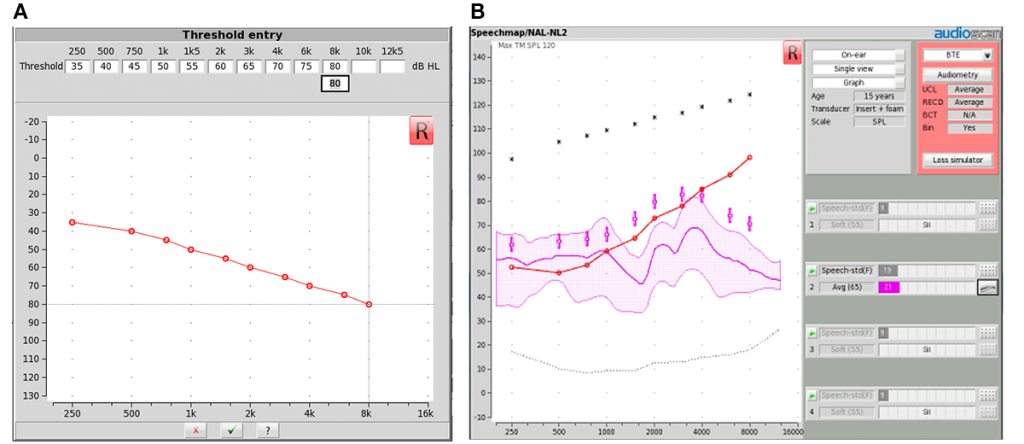
Figure 3. Example of a real-ear aided response (REAR) measurement on a SPL-o-gram or Speechmap screen, obtained with an average speech input levels. Also shown are the REAR targets generated by the prescriptive formula for that particular input level (+’s), the patient’s thresholds (X’s) and the predicted UCLs for the patient (*’s).
Furthermore, given the previously mentioned concerns regarding the relative impact of direct versus indirect sound paths in an open fitting, this approach inherently provides a representation of both signal paths simultaneously and offers an ability to assess whether or not the output seems appropriate relative to the selected fitting formula targets – or the patient’s dynamic range. Questions regarding which REUG to use (i.e., average or measured) are no longer an obstacle with the REAR approach as we are solely interested in the SPL level required at the eardrum to meet the target criteria.
Transparency of the open dome can sometimes lead to questions regarding the impact of open fitting acoustics on insertion gain approaches which use the REUR/G as part of their target calculation as mentioned above. In this respect, it should be noted that just because a product or coupling is labeled as “open” it does not necessarily mean that particular device provides ‘open acoustics’ in the ear canal. The author has come across cases where the coupling diameter selected by the clinician was too large for the ear canal in question, leading to a more occluded fitting than might otherwise be anticipated. In this regard, a quick real-ear occluded response (REOR) measurement can serve as a handy tool to accurately determine the acoustic realities of the vent condition relative to the open ear canal (see Figure 4). Simply conduct a REM with the hearing instrument in place and turned off and then compare the resulting measurement to a previously measured REUR using the same input signal. Should the 2 curves (REOR and REUR) overlap, evidence of an open fitting is present – and open fitting verification considerations would apply.
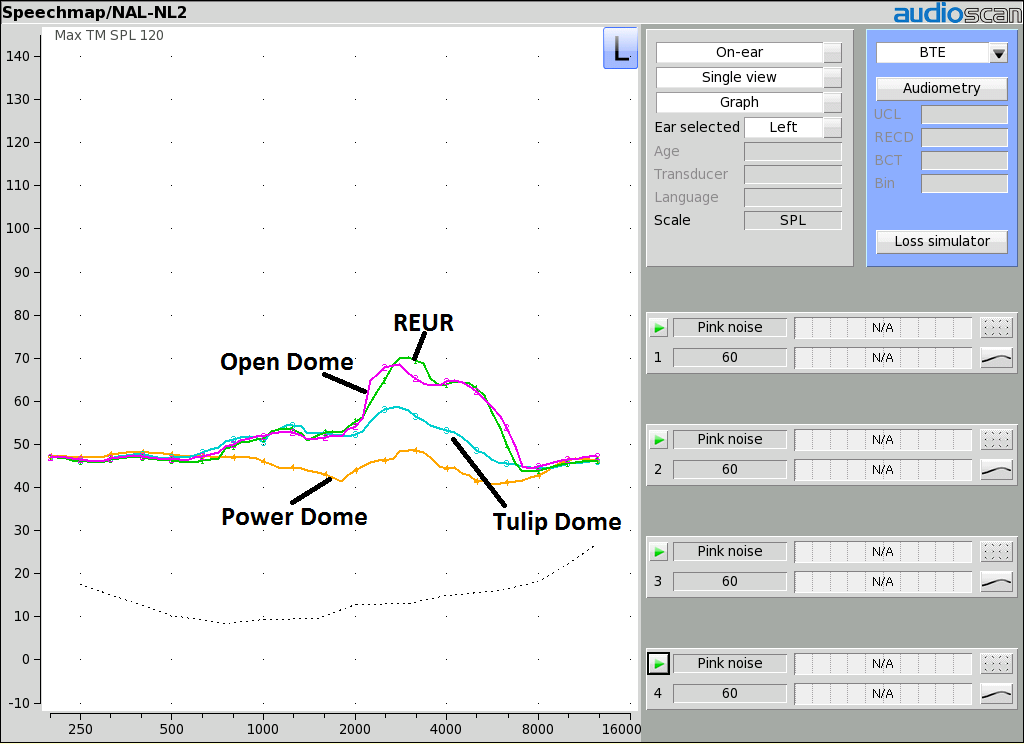
Figure 4. Example of real-ear occluded response (REOR) measurements for various device venting conditions. Shown is the previously measured REUR, along with REOR measurements for an open dome, tulip/closed dome and a power/occluding dome. Note the reduction in the measured response relative to the REUR as the venting is gradually decreased and the ear canal becomes more occluded.
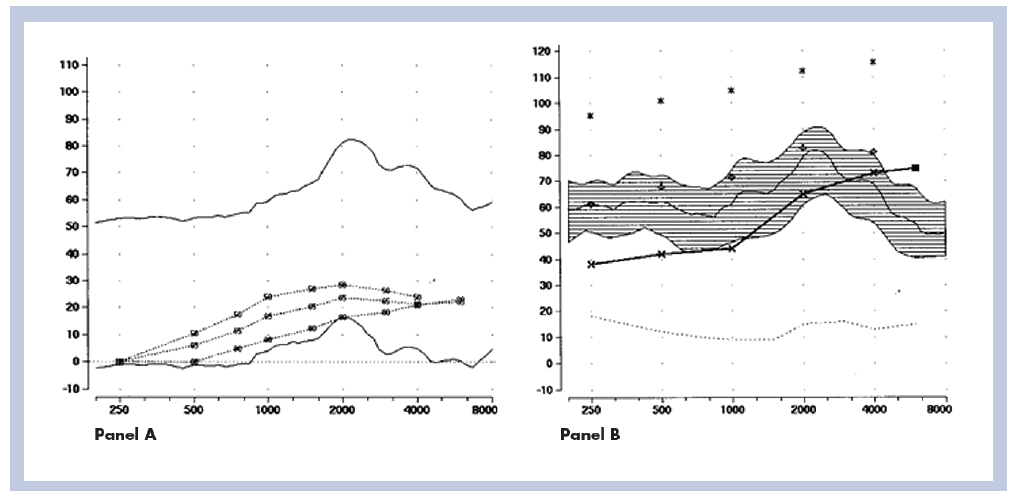
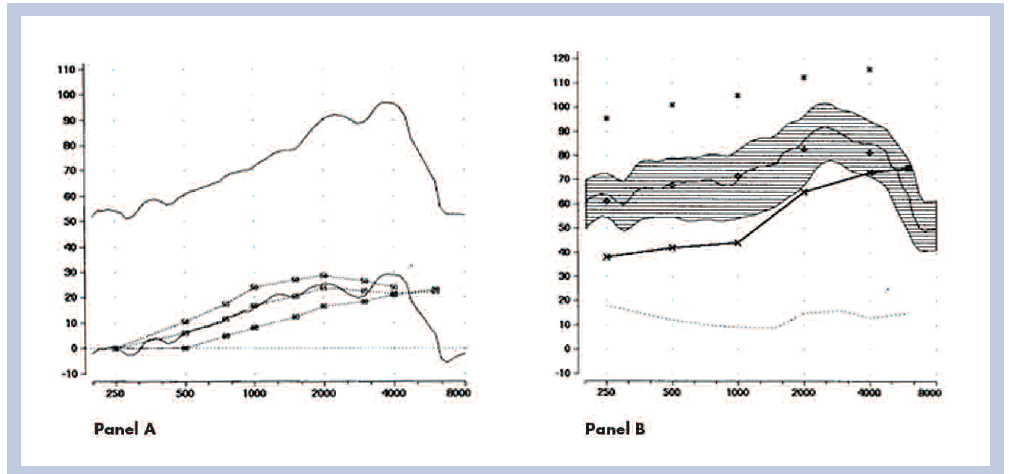
The aforementioned differences in the verification methods described above has understandably led some to question how REMs might compare should an REIG versus an REAR approach be used to fit open devices. While there appears to be limited data on the subject, Mueller and Ricketts reported that, while the REAR approach is typically recommended, either approach can be used for fitting of open products, and that the conclusions from either method for target matching should be equivalent.13 In that regard, Mueller & Ricketts show example fittings where a quick fit resulted in a poor target match using either the REIG or the REAG approach (see Figure 5)13; and when adjusted to target, a good match was observed with either the REIG or REAR approach (see Figure 6).
Similarly, Bentler et al. indicate that you should expect to see similar match to targets with either the Insertion Gain or REAR approach, with the exception being patients with an unusual REUG. In this case, it is advised that one would default to the average REUG provided by a number of REM systems.14
Ultimately it is unclear for the individual patient how an unusual REUR might impact this relative relationship in target matching outcomes between the REIG and REAR approaches. Consider that, given how the REIG is calculated, that the difference between the REUR and the REAR determines how much additional gain is needed in a product fitting. Consider also that ultimately what we listen to is output at the eardrum, not gain. The logical challenges associated with including an REUG that was not part of the assessment in the determination of required output at the eardrum has led some to suggest that the REAR approach is the fitting method of choice. That is, by moving to the REAR philosophy, questions involving the REUG not being part of the assessment, which REUG to use (average or measured) and whether or not the average REUG is appropriate can all be addressed by focusing on the REAR approach. The fitter can then leverage all of the other relative benefits that this technique has to offer compared to the REIG method as described above. Further, all of these verification benefits can be had with one fewer measurement as the REUG does not need to be conducted.
As it relates to fitting formula targets, even if one aligns themselves with the REAR philosophy, there has been some confusion regarding the need for different targets for open fittings versus other coupling conditions. Part of this confusion may relate to consideration of 2cc coupler versus real-ear targets. No doubt, coupler targets do need to change as a function of the form factor and venting characteristics, primarily for the lower frequencies. Also, as expressed by a number of researchers and REM manufacturers, the ability to accurately simulate an open fitting in the test box is limited at the present time, given the inability to accurately simulate venting in test box measures. As such, REM systems typically disallow simulated real-ear (i.e., coupler-based) measurements to targets with open fit products.
However, as pointed out by multiple authors,13,15 REM targets do not change with the openness of the fitting. Ultimately we are concerned with the signal level required at the eardrum when matching REM targets and while the openness of the fit may impact sound quality,16,17 in regards to target matching it arguably does not matter how the signal gets to the eardrum – be it via the direct-vent transmitted path, via the indirect amplified path or some combination thereof. While questions have arisen regarding summing and cancelling effects between the direct and indirect sound paths, Mueller and Ricketts have pointed out that these factors are largest when the hearing instrument is providing little to no gain and are not expected to play a major role in achieving desired REM targets.13
Now, while I am personally a big proponent of the REAR approach as it relates to open fitting products, value for the REUR measurement with this coupling condition can be found in areas such as: (1) documenting the openness of the fitting (as highlighted in Figure 4); and (2) documenting whether or not someone is actually a candidate for an open fitting in the first place. A simple comparison of an REUR measurement (or REOG where the hearing instrument is in place, turned off with the probe tube in place) to the patient’s thresholds and/or the selected fitting formula targets for the selected input level in the SPL-o-gram view can quickly reveal whether or not sufficient audibility is provided with direct sound travelling down the ear canal in the low frequency region. An example of this approach is shown in Figures 7 and 8.
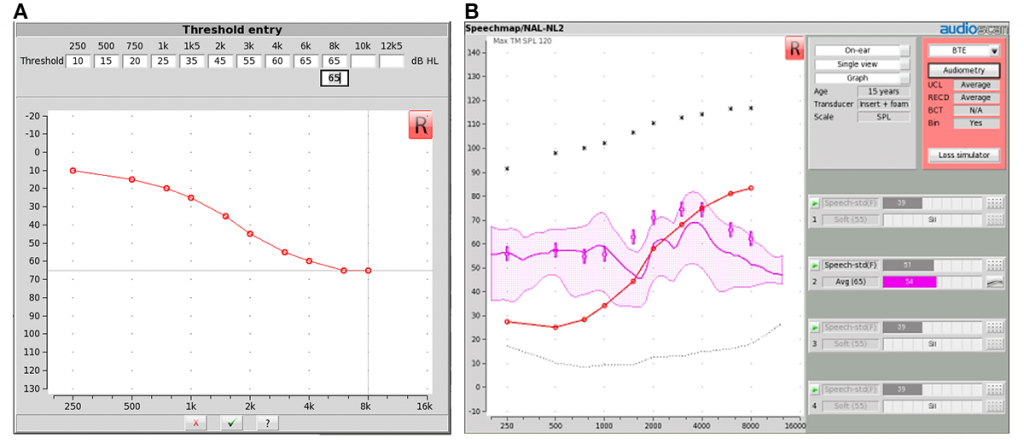
Figure 7 shows a dB HL audiogram for one individual, subsequently converted into a dB SPL format and then plotted alongside an REUR measurement conducted using average speech. We can observe that the long-term average value of the REUR measurement (i.e., the centre thick pink line in the shaded speech spectrum) closely approximates the generated prescriptive targets in the low frequency region up to approximately 1 kHz. A finding such as this one suggests that the direct sound path would provide sufficient audibility for the patient in question in the low frequency region where the hearing instrument would not be capable of delivering audibility due to venting.18 As a result, this individual would be considered a typical candidate for an open fit device.
Figure 8 shows a dB HL audiogram for another individual with more significant low frequency hearing loss – converted into the dB SPL format once again and then plotted alongside another REUR measurement. We can observe in this case that the direct sound path (i.e., the REUR represented by the centre thick pink line in the shaded speech spectrum) is not providing sufficient audibility relative to the generated low frequency region up to approximately 1 kHz. In contrast to Figure 7, a result such as this suggests the patient in question is not a candidate for an open fitting and would likely require a more occluding fitting to ensure that the required level of low frequency amplified sound is not vented out of the ear canal and is instead delivered to the eardrum.18
Regardless of the fitting approach selected (REIG or REAR), there is one significant difference in verification with open fittings relative to more occluded fittings that needs to be captured to increase the likelihood of accurate REMs. This consideration relates to the manner in which the sound field is calibrated (or ‘equalized’). Specifically, when conducting verification with open fit products the amplified signal being generated by the hearing instrument can leak out of the ear canal and be picked up by the reference microphone (see Figure 9), creating errors in the sound field calibration routine and any resulting REM.
The reference microphone serves to monitor the input signal level during REM and adjusts the speaker level to ensure that the requested input signal and spectrum is delivered to the measurement location. Traditionally, on most REM systems, the reference microphone remains active during testing, using what is termed the “concurrent modified pressure method of equalization.” This approach works well for most fittings, as it will adjust the signal level generated by the loudspeaker should the patient move during testing to always ensure the correct signal level/spectrum is delivered to the measurement point. However, with open fittings, the amplified sound leaking from the ear canal can be picked up by the reference microphone in addition to the speaker signal. In these cases, the REM system will “see” a greater input signal and turn down the speaker level, resulting in a signal level lower than it otherwise would have been had the measurement artifact not occurred. Figure 10 shows the potential impact of this artifact, whereby an open fit product was measured twice with the exact same hearing aid settings using different sound field calibration methods. First, REM was conducted with the reference microphone active throughout testing (the ‘concurrent modified pressure method of equalization’). Afterwards, the device was again measured using the ‘stored modified pressure method of equalization’ where the reference microphone remains off during REM. With this stored calibration approach, the sound field is calibrated once with the patient in the test location and the hearing aid muted, and then following activation of the hearing aid for testing, the reference microphone remains off.
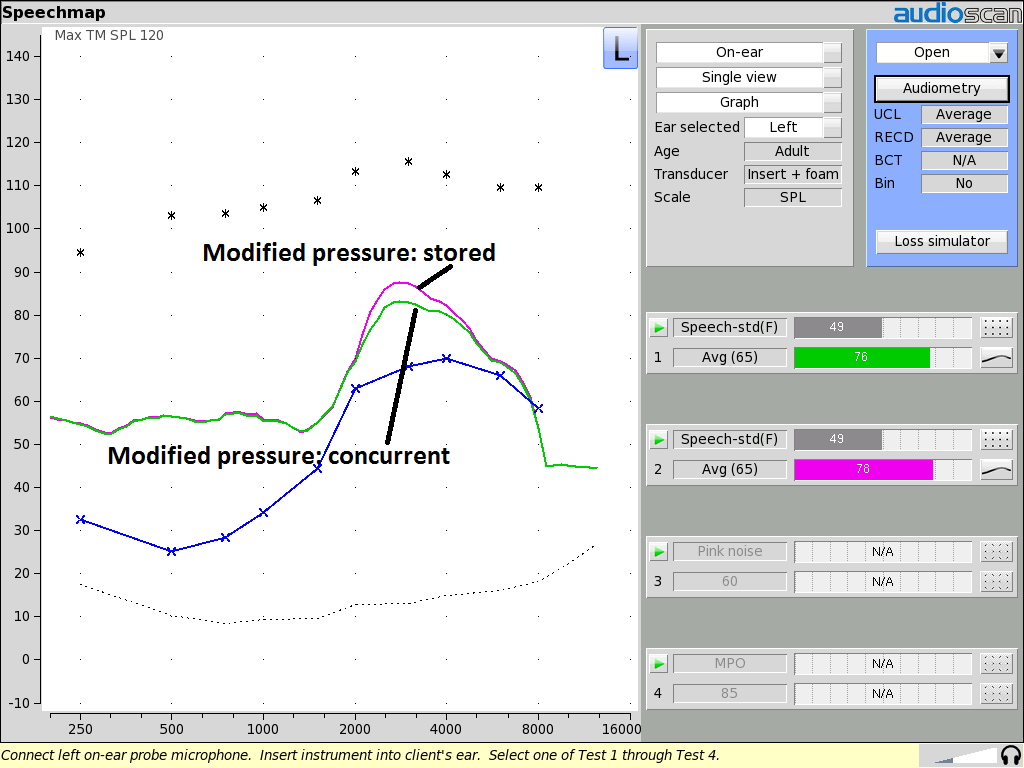
Figure 10. Example of REARs for average speech for the same patient, using the same open fit hearing aid at the exact same settings for: a) the modified pressure method ‘stored’ equalization approach; and b) the modified pressure method ‘concurrent’ equalization approach. Note that the concurrent equalization measurement is lower than the stored equalization due to contamination from vented amplified sound during the calibration routine.
It doesn’t take much of a leap to surmise that the artifact in this example might lead a clinician to unnecessarily increase high frequency gain/output in a hearing instrument – say for example if they are under fitting targets. An under fitting may simply relate to the input signal level being lower than required as the vented amplified signal has resulted in the REM system turning down the loudspeaker. It would probably then not be too surprising that such a patient might report that a device subsequently set to targets is now too loud, sharp or tinny. If the proper input level had been provided, the device would have revealed greater output, which may have led to entirely different programming decisions. To ensure that conclusions are accurate and subsequent programming is appropriate with open fittings, it is important to use the stored modified pressure equalization approach. Thankfully most measurement systems provide a method of capturing this automatically for you. Simply select ‘open’ as the device type / venting condition from the REM system software menu. In most REM systems, this selection results in the equipment taking you through a procedure which stores the sound field calibration at the measurement point with the hearing aid muted (see Figure 11). Provided the patient does not move from the previously calibrated position, the fitter can be certain the proper input signal level/spectrum is delivered to the hearing instrument.

Figure 11. Example of a stored modified pressure method equalization prompt provided by one manufacturer upon beginning REM with an open fit device.
Summary
Verification of hearing instruments brings with it a number of benefits, both to clinicians and to patients. As expressed above, there are a number of considerations to keep in mind when conducting REM with Open fittings, regardless of whether one subscribes to the insertion gain or real-ear aided response camps. That said, general fitting principles with open fittings remains in large part the same as with any other hearing instrument coupling condition – the required SPL level at the eardrum for the hearing loss in question is the same regardless of how that signal level arrives at the eardrum – via the vent, via the hearing aid, or some combination thereof. While insertion gain remains the option of choice for some clinicians, REMs via the real-ear aided response / SPL-o-gram technique outlined above offers significant relative advantages allowing one to quickly capture the combined impact of both signal paths and their influence on all relevant prescriptive fitting and dynamic range variables at all points in the fitting.
References
- Aazh H, Moore BC. The value of routine real ear measurement of the gain of digital hearing aids. J Am Acad Audiol 2007 Sep;18(8):653–64.
- Aazh H, Moore BC, Prasher D. The accuracy of matching target insertion gains with open-fit hearing aids. Am J Audiol 2012;21(2):175–80. doi: http://dx.doi.org/10.1044/1059-0889(2012/11-0008)
- Mueller HG. 20Q: Real-ear probe-microphone measures—30 years of progress? AudiologyOnline, Article 12410 [Jan 2014]. Available at: http://www.audiologyonline.com
- Sanders J, Stoody TM, Weber JE, Mueller HG. Manufacturers’ NAL-NL2 fittings fail real-ear verification. Hear Rev 2015;21(3):24–30.
- Amlani AM, Pumford J, Gessling E. REM and its impact on aided audibility and patient loyalty. Hear Rev 2017;24(10):12–21.
- Abrams HB, Chisolm TH, McManus M, McArdle R. Initial-fit approach versus verifiedprescription: comparing self-perceived hearing aid benefit. J Am Acad Audiol Nov/Dec, 2012;23(10):768–78.
- Leavitt R, Flexer C. The importance of audibility in successful amplification of hearing loss. Hear Rev 2012;19(13):20–23.
- Valente M, Odeing K, Brockmeyer A, Smith S, Kallogjeri D. Differences in word and phoneme recognition in quiet, sentence recognition in noise, and subjective outcomes between manufacturer first-fit and hearing aids programmed to NAL-NL2 using real-ear measures. J Am Acad Audiol 2017. doi.org/10.3766/jaaa.17005
- Mueller GH. Probe-mic measures: Hearing aid fitting’s most neglected element. Hear J 2005;58(10):21–30. doi: 10.1097/01.HJ.0000285782.37749.fc
- Mueller HG, Picou EM. Survey examines popularity of real-ear probe-microphone measures. Hear J 2010;63(5):27–32.doi: 10.1097/01.HJ.0000373447.52956.25
- Mueller HG. Terminology and Procedures. In: Mueller HG, Hawkins DB, Northern JL, editors. Probe Microphone Measurements. San Diego: Singular Publishing; 1992
- Revit LJ. An open letter: New thinking on the proper application of REMs to prescriptions and fittings. N Z J Audiol 1991;1:1–17.
- Mueller HG, Ricketts TA. Open-canal fittings: ten takehome tips. Hear J 2006;59(11):24–39.
- Bentler R, Mueller HG, Ricketts TA. Probe microphone clinical uses. In: Bentler, Mueller, Ricketts (eds.): Modern Hearing Aids: Verification, outcome measures, and follow-up. San Diego, CA: Plural Publishing, Inc.; 2016.
- Dillon H. Hearing Aids. Turramurra, Australia: Boomerang Press; 2001.
- Kuk F. Perceptual consequences of vents in hearing aids. Br J Audiol 1991;25(3);163–69.
- Kuk F, Keenan D. How do vents affect hearing aid performance? Hear Rev 2006 Feb;13(2):34.
- Smriga D. On ear verification of open fittings. AudiologyOnline, Article 19326; 2017. Available at: http://www.audiologyonline.com.