To the Brain and Back

Misophonia and the Brain
Misophonia – meaning “hatred of sound” – describes when a person experiences extreme emotions, such as distress, anger, and disgust, in response to certain sounds. Sound types that “trigger” misophonia are numerous, but the most common are associated with orofacial movements, such as chewing, swallowing, and other mouth noises. Other common triggers include pen clicking, leg shaking, or the clinking of dishware. Although many people find these sounds unpleasant or mildly annoying, about 5% of the population experience debilitating misophonia that rises to clinically significant levels.1,2 In these cases, exposure to trigger sounds can induce feelings of intense rage, desperation, and even thoughts of self-harm.
Misophonia is distinct from hyperacusis when normal everyday sounds are unbearably and painfully loud. In misophonia, the source or meaning of the sound is intolerable, not the perceived loudness. In addition, misophonia often arises when pure-tone thresholds are normal; therefore, hearing loss is not a reliable risk factor.
Although misophonia is not currently classified as a disorder in diagnostic resources such as the DSM, it is often comorbid with other psychological conditions such as depression and anxiety disorders. There are no widely established treatments; however, cognitive behavioural therapy and sound therapies are commonly used in addition, to trigger sound avoidance.3 Pharmacological treatments and brain stimulation therapies are also under investigation as possible routes for intervention.4 In Canadian Audiologist, Glynnis Tydball recently wrote about two misophonia cases (2020, vol. 7 issue 1). The article provides an insightful patient perspective detailing the emotional toll on families, and ultimately calls for compassion and accommodation for people with misophonia.
One ongoing debate considers whether misophonia is an auditory disorder and, therefore, of concern to audiologists, or whether it is a neurological issue outside of hearing science. To unpack this issue, I will discuss three proposed neural bases of misophonia: emotional, social, and motor (movement) factors. Note that the term misophonia was only coined in 2002,5 and the available neuroscience literature is quite recent.
Emotional Hyperactivity Hypothesis
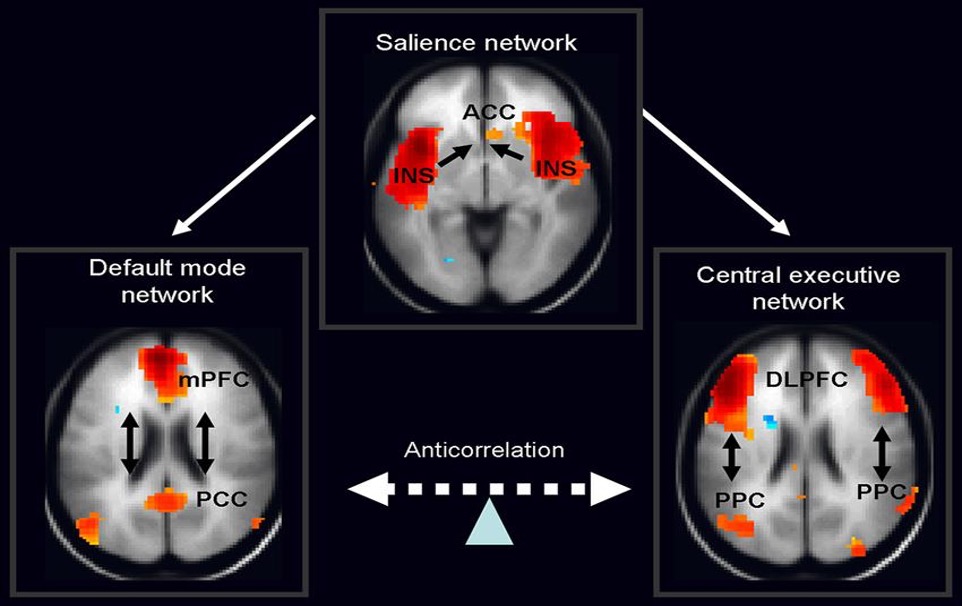
One explanation for misophonia is that it arises from hyperactivity in a brain network involved in cognition and emotional evaluation. The “salience network” (Figure 1) integrates and evaluates important or “salient” events that a person experiences, including their emotional meaning.6 The network includes major hubs in the anterior insula and anterior cingulate cortex. It is thought to control whether the brain is focused on networks responsible for “inner” or internal mental states (the default mode network) or networks that process external events and behavioural goals (the central executive network).
Interestingly, studies report that trigger sounds elicit stronger salience network activation in people with misophonia, which may drive physiological distress. In one paper, Kumar et al.,8 used functional magnetic resonance imaging (fMRI) and found that misophonic trigger sounds increased activity and connectivity within the anterior insula and anterior cingulate, the hubs of the salience network. This neural activity was correlated with participants’ behavioural ratings of their misophonia, and explained increases in heart rate and skin conductance (sweat gland activity), consistent with sympathetic arousal. Another study found that participants with misophonia have enlarged amygdalae, which are core emotion-processing regions in the brain.9,10 Interestingly, the auditory cortex did not show evidence for hyperactivity, suggesting that the aberrant responses in misophonia involve higher-level cognitive processes rather than lower-level sensory activity.
Motor Hypothesis
A more recent hypothesis proposed by Kumar and colleagues11 suggests that misophonia may have a motor origin. Since many misophonic triggers involve orofacial movements, the authors predicted that people with misophonia may have an overactive “mental mirroring” or internal mimicry of orofacial movements, which could drive extreme emotional responses. In other words, the brain areas responsible for controlling facial movements like chewing and swallowing become hyperresponsive, not the areas that process sounds. Motor activation in the brain could possibly drive stronger responses in the salience network. In support of this explanation, the authors found that triggering sounds increased activity in the orofacial motor area of the brain in participants with misophonia. People with misophonia showed increased connectivity between motor areas and auditory cortex, suggesting increased processing for sound perception's motor aspects. Other fMRI studies also report motor and premotor brain activation in those with misophonia,12 further supporting the motor hypothesis.
Social Cognition Hypothesis
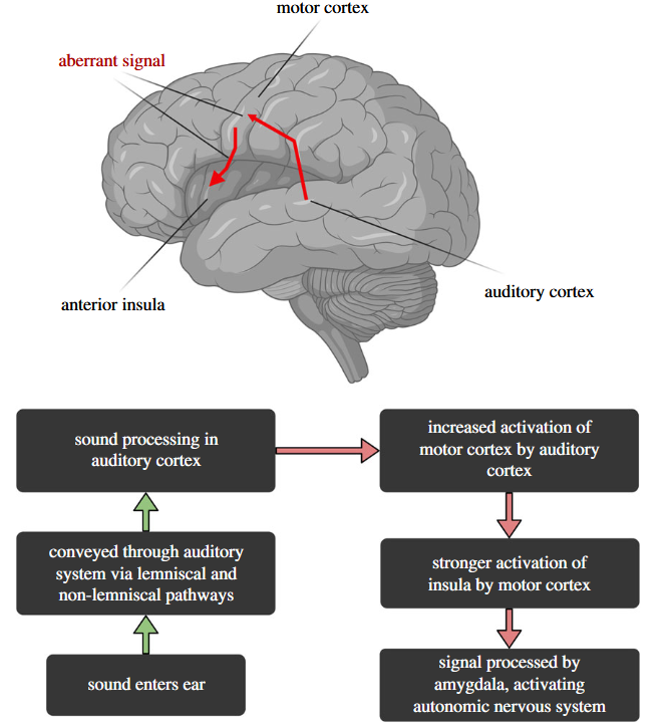
A final explanation for misophonia considers the social context in which misophonia commonly occurs. Orofacial or manual sound triggers, such as chewing, swallowing, or pen clicking, are mainly produced by people, meaning the experience of misophonia typically arises during social interactions. Interestingly, studies show that family members or other familiar people, rather than strangers or less familiar people, induce stronger misophonia responses when they produce trigger sounds.13 These findings highlight that the source of the triggering sound may be as important as the sound itself within a social and emotional context. Berger and co-authors14 propose a social cognition model that integrates the previous hypotheses for emotional hyperactivity and motor mimicry within a social framework (Figure 2). The social cognition model reconsiders the role of the anterior insula, which was recently shown to play a major role in social evaluation and emotions [15]. In Berger and colleagues’ combined model, trigger sounds are processed normally by the auditory system, but generate aberrant neural activity in the motor system via increased mimicry. Aberrant signals pass from the motor structures to the insula and amygdala that process the larger socio-emotional context. The insula in turn, could activate brain areas involved in sympathetic arousal, resulting in an intense physiological distress response.
The neuroscience insights above do not suggest that misophonia originates through sound perception or hearing function alone. From this angle it is difficult to argue that misophonia is solely an auditory problem. As such, there is debate about whether misophonia is an audiology, neurology, or psychiatry issue.10 Despite this, many people experiencing misophonia will initially contact audiologists or request ENT referrals, believing they are experiencing a hearing problem. Hearing healthcare specialists are the first point of care in these cases, and begin important steps such as building a case history and providing initial hearing care. This motivates the need for audiological consensus on diagnostic assessment and treatment for misophonia.16 In addition, some useful questionnaires are available for clinicians, such as the Duke Misophonia Questionnaire.17 In the long term, the right care team might require coordination between hearing specialists and neurological and psychiatric professionals in a patient-specific manner.
References
- Dixon, L. J., Schadegg, M. J., Clark, H. L., Sevier, C. J., & Witcraft, S. M. (2024). Prevalence, phenomenology, and impact of misophonia in a nationally representative sample of US adults. Journal of psychopathology and clinical science.
- Jakubovski, E., Müller, A., Kley, H., de Zwaan, M., & Müller-Vahl, K. (2022). Prevalence and clinical correlates of misophonia symptoms in the general population of Germany. Frontiers in psychiatry, 13, 1012424.
- Mattson, S. A., D’Souza, J., Wojcik, K. D., Guzick, A. G., Goodman, W. K., & Storch, E. A. (2023). A systematic review of treatments for misophonia. Personalized medicine in psychiatry, 39, 100104.
- Neacsiu, A. D., Szymkiewicz, V., Galla, J. T., Li, B., Kulkarni, Y., & Spector, C. W. (2022). The neurobiology of misophonia and implications for novel, neuroscience-driven interventions. Frontiers in Neuroscience, 16, 893903.
- Jastreboff, M. M., & Jastreboff, P. J. (2002). Decreased sound tolerance and tinnitus retraining therapy (TRT). Australian and New Zealand Journal of Audiology, The, 24(2), 74-84.
- Seeley, W. W. (2019). The salience network: a neural system for perceiving and responding to homeostatic demands. Journal of Neuroscience, 39(50), 9878-9882.
- Nekovarova, T., Yamamotova, A., Vales, K., Stuchlik, A., Fricova, J., & Rokyta, R. (2014). Common mechanisms of pain and depression: are antidepressants also analgesics?. Frontiers in behavioral neuroscience, 8, 99.
- Kumar, S., Tansley-Hancock, O., Sedley, W., Winston, J. S., Callaghan, M. F., Allen, M., ... & Griffiths, T. D. (2017). The brain basis for misophonia. Current Biology, 27(4), 527-533.
- Eijsker, N., Schröder, A., Smit, D. J., van Wingen, G., & Denys, D. (2021). Structural and functional brain abnormalities in misophonia. European Neuropsychopharmacology, 52, 62-71.
- Aryal, S., & Prabhu, P. (2023). Understanding misophonia from an audiological perspective: a systematic review. European Archives of Oto-Rhino-Laryngology, 280(4), 1529-1545.
- Kumar, S., Dheerendra, P., Erfanian, M., Benzaquén, E., Sedley, W., Gander, P. E., ... & Griffiths, T. D. (2021). The motor basis for misophonia. Journal of neuroscience, 41(26), 5762-5770.
- Cerliani, L., & Rouw, R. (2020). Increased orbitofrontal connectivity in misophonia. BioRxiv, 2020-10.
- Bell, B. M., Spruijt-Metz, D., Vega Yon, G. G., Mondol, A. S., Alam, R., Ma, M., ... & De la Haye, K. (2019). Sensing eating mimicry among family members. Translational behavioral medicine, 9(3), 422-430.
- Berger, J. I., Gander, P. E., & Kumar, S. (2024). A social cognition perspective on misophonia. Philosophical Transactions of the Royal Society B, 379(1908), 20230257.
- Lamm, C., & Singer, T. (2010). The role of anterior insular cortex in social emotions. Brain structure and function, 214, 579-591.
- Campbell, J. (2023). Misophonia: A Need for Audiological Diagnostic Guidelines. Journal of the American Academy of Audiology, 34(07/08), 176-180.
- Rosenthal, M. Z., Anand, D., Cassiello-Robbins, C., Williams, Z. J., Guetta, R. E., Trumbull, J., & Kelley, L. D. (2021). Development and initial validation of the Duke Misophonia Questionnaire. Frontiers in psychology, 12, 709928.