The Mysterious Cartilaginous/Bony Ear Canal Junction

Wayne Staab, PhD (Trends) was one of the first audiologists to work with manufacturers back in the 1970s and has a wealth of both historical and current knowledge. His perspectives are balanced and always well thought out.
Research related to the occlusion effect (OE) suggests that the OE is minimized when contact of the ear insert (closed coupled in this case) is made with the bony ear canal.1,2 Measurements of the OE for various in-canal devices are numerous and essentially support this conclusion.
However, what is NOT clear from anatomical references of the ear canal is just where and how this delineation between the two takes place. And, what would the impact on the OE be by contact of the in-canal device with the bony structure of the ear canal, either partially or complete? This article will not attempt to answer the latter part of the previous question, but instead will concentrate on the delineation issue.
What Textbooks Tell Us
Interestingly, text books vary in this delineation, but most say that the approximate outer third of the ear canal is lined primarily by cartilage, and the approximate inner two thirds by bone. Unfortunately, essentially none of these sources provides actual information/measurements. Instead, they quote other sources, who also provide no actual information/measurements. Certainly, ear surgeons, especially those that specialize in outer ear surgeries understand the anatomical delineations, but it is difficult to find sources that report specifically on this transition from cartilaginous to bony canal wall structure.
Ear Canal Isthmus
One issue where there seems to be some consistency, is that the transition occurs at the isthmus of the ear canal. But, how far in from the ear canal aperture is the isthmus? Is it positioned somewhat similar in all individuals, or does it vary dramatically? And, how much of the ear canal is encased by bone at this transition point?
Data from the only studies this author has found that places a measurement number on the location of the isthmus is found in Figure 1.3–5 They show the average distance of the isthmus from the canal aperture to be 9.53 mm. Even though the ear canals are of different lengths, the isthmus measurement from the canal aperture does not vary as widely as some might suspect. This holds true even for the very short ear canal (23 mm) where the isthmus is below the average by only 1.53 mm – a very small deviation. The entire range of isthmus location is only 2.8 mm.
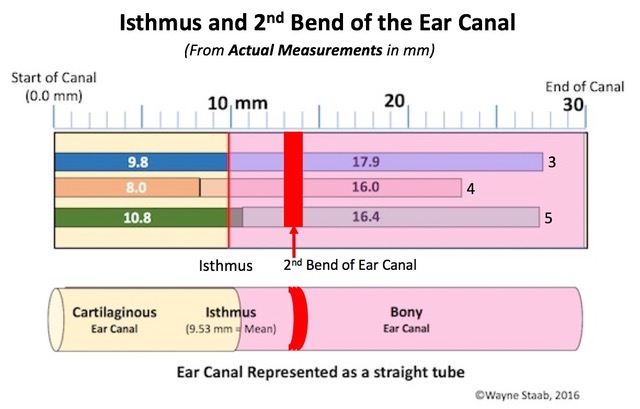
Figure 1. Location of the isthmus and 2nd turn of the ear canal from actual measurements (in mm) from the aperture (opening) of the ear canal. The numbers 3, 4, and 5 at the end of each of the canal measurements refer to the same numbers in the references.
Some have suggested that the differentiation between the bony and cartilaginous canal can be visualized by looking carefully at ear impressions to determine if there are skin pore markings, which would provide evidence of the cartilaginous canal, or if there are no pore markings, but smooth, an indication of the bony portion of the ear canal.6,7 Skin pore areas represent portions of the ear canal having subcutaneous structure that allows for sebaceous or ceruminous glands and/or hair follicles to show. Checking for this difference requires that the ear impression be made with low viscosity (runny), a high-quality silicone low Shore A hardness impression material, and use of a high-quality microscope. The problem is that this is a totally subjective evaluation. And even then, only 9% of the ear impressions provided sufficient information to make an estimated decision of 100% completely bony covering.7 Additionally, the ear impression must be of sufficient length to show both the bony and cartilaginous ear canal areas.
Skull Anatomy
What is known is that the bony anatomy of the skull (specifically the temporal bone) provides some useful information about this transition area from cartilage to bony ear canal underlying structure.
The ear canal is entirely encased by the temporal bone closer to the tympanic membrane (TM). But, the temporal bone has a bony shelf (Figure 2) at the inferior portion that can extend well into, and even past the isthmus area of adults, even shown as close as about 7 mm to the canal aperture.
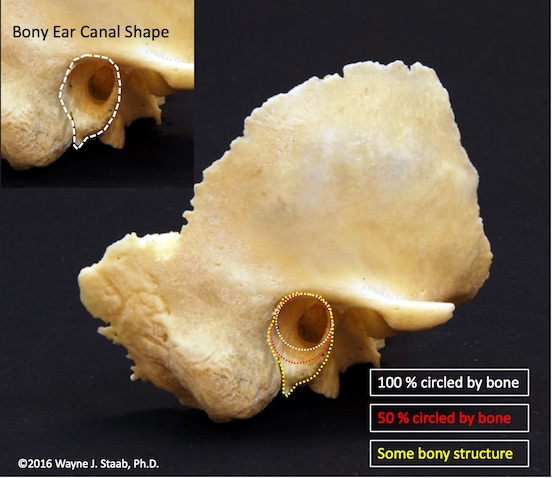
Figure 2. The bony enclosure of the ear canal extends well into, and even lateral to the second bend in adult ear canals, possibly enclosing the isthmus area in some individuals. It is tempting for some to conclude that the cartilaginous canal extends from the aperture of the ear canal to the complete encasement in bone, but it is just as logical to contend that the bony portion extends from the tympanic membrane to where there is no bony substructure, meaning possibly to, and even beyond, the isthmus. In either case, the average complete enclosure (100%) extends essentially to the second bend of the ear canal. The most lateral extension of the bony shelf can be to within 7.6 mm of the ear canal aperture.
Parasagittal plane computed tomographic (CT) images (0.6 to 1 mm slice thicknesses) were measured on 62 ears of subjects older than 18 years of age. As measured from the annulus (attachment of the TM to the bony canal wall), the osseous external auditory canal showed an average complete enclosure by bone out to 9.8 mm, with a range from 4 to 17.4 mm.8 This means that the bony canal is complete to essentially the second bend (Figure 1) of the ear canal in most individuals, with varying degrees of completeness extending outward from that region.
What Does This Mean?
What this all means is that for many individuals, the need to extend the hearing aid coupling seal well beyond the second bend to minimize the occlusion effect may not be necessary to help minimize this effect. Additionally, the cartilaginous/osseous relationship of the ear canal is clearer than presented previously in generalized terms.
References
- Zwislocki J. Acoustic attenuation between the ears. J Acoust Soc Am 1953;25, 752–59.
- Killion MC, Wilber LA, Gudmundsen G. Zwislocki was right...a potential solution to the “hollow voice” problem the amplified occlusion effect with deeply sealed ear-molds. Hear Instrum 1988;39:14–18.
- Ahmad I, Lee WC, and Binnington JD. External auditory canal measurements localization of the isthmus. Oto-Rhino-Laryngologia Nova 200010(5):283–86.
- Gray H. Anatomy of the Human Body. Dudley, UK: Bartleby.com, Inc; 2000.
- Tu HS, Yu JF, Wang RH, Chen YS. Anthropometry of external auditory canal by non-contactable measurement. Center for Measurement Standards, Industrial Technology Research Institute, Taiwan, and Taiouan Interdisciplinary Otolaryngology Laboratory, Chang Gung University, Taiwan. Noise 2014, Melbourne Australia, 16-19, November; 2014
- Nielson C. and Darkner S. The cartilage bone junction and its implication for deep canal hearing instrument fittings, Hearing J 2011;64(3)35-36,40,42.
- Oliveira RJ, Hoeker R: Ear canal anatomy and activity. Sem Hear 2003;24(4):265–75.
- Mahboubi H, Wu EC, Jahanbakhshi R, et al A novel method to determine standardized anatomic dimensions of the osseous external auditory canal. Otol Neurotol. 2012;33(5):715–20. doi: 10.1097/MAO.0b013e3182544e55.