Mysteries of the Hearing Brain: What is Normal Hearing?

A 63-year-old woman scheduled an appointment for an audiological evaluation because she has observed hearing difficulty in noisy environments. Her mother has a mild-to-moderate sensorineural hearing loss that has slowly progressed over the last 25 years, and she has been wearing hearing aids successfully since the age of 62. The patient’s father has a military service-related hearing loss and has been wearing aids for over forty years. This patient is interested in learning if she is a hearing aid candidate or any other options to help her hear in challenging environments. She is a professor at a large university and notices particular difficulty hearing in conferences, restaurants, and in large classrooms. She has no history of ear infections. The audiological exam revealed normal hearing sensitivity through 4000 Hz, dropping to a mild sensorineural hearing loss at 6000-8000 Hz bilaterally. Immittance measures revealed normal middle ear function bilaterally. Word recognition ability was excellent bilaterally. She was told that she has normal hearing and that everyone has trouble hearing in noisy backgrounds. No recommendations for management were provided.
Does this sound like a familiar scenario? I have given the same feedback to patients with similar profiles. Yet, the patient’s complaints were not addressed. This particular patient happens to be me. I know that I have more difficulty hearing noise than my younger students and relatives. I often ask them to repeat what they or others have said. So perhaps my hearing ability is normal for my age, but not normal relative to younger listeners.
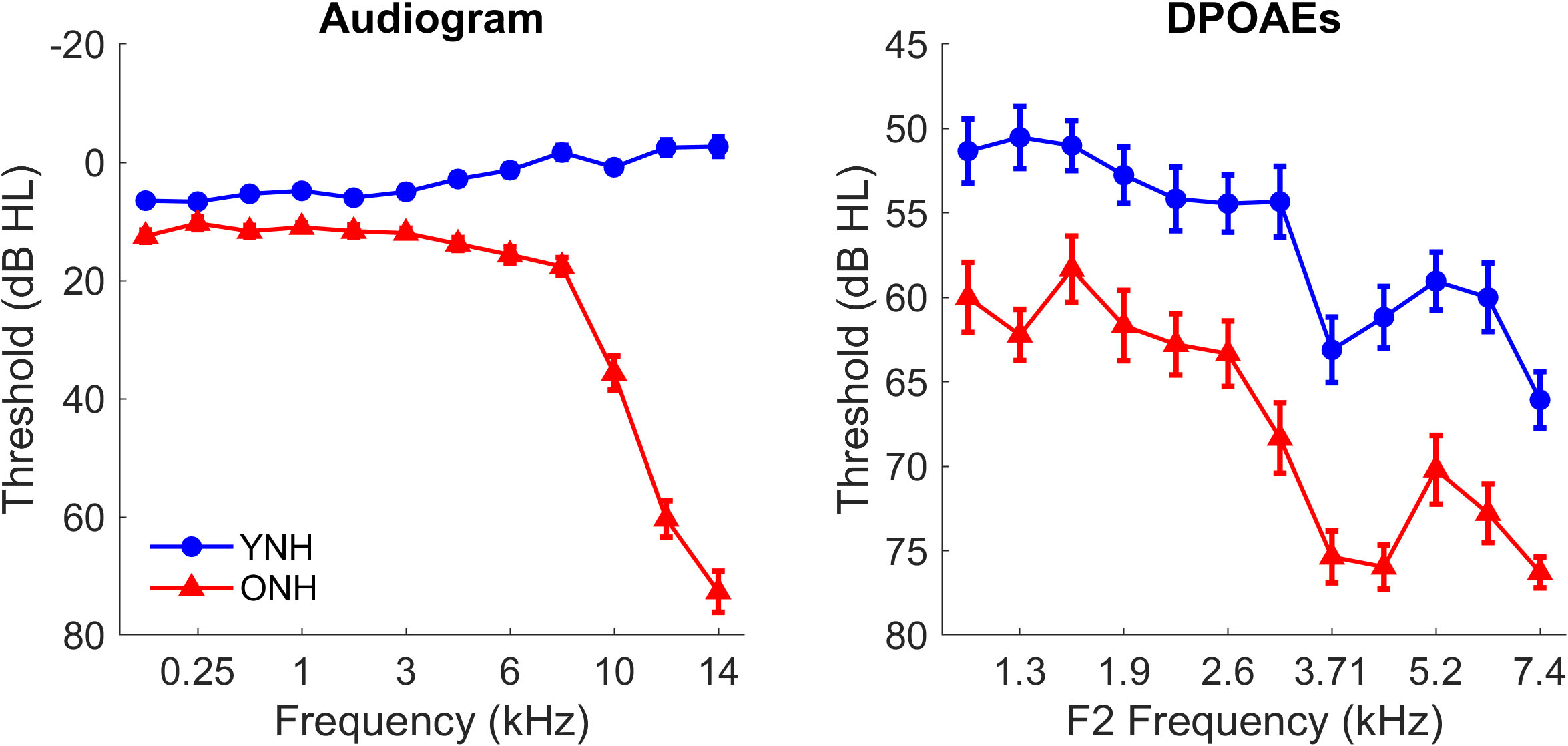
We know a wide range of “normal” thresholds on the audiogram – anywhere from -10 to 20 dB HL – a 30 dB range! Indeed, an individual with hearing thresholds of 15-20 dB has more difficulty hearing than an individual with hearing thresholds of 0-5 dB. Are there upstream effects of slightly decreased thresholds at higher levels of the auditory system? We recently published the results of a study that investigated the effects of slight peripheral deficits on neural processing in individuals with clinically normal hearing (thresholds ≤ 20 dB HL).1 Figure 1 displays audiometric and distortion product otoacoustic emissions (DPOAEs) thresholds in younger and older listeners who met this criterion. Note that thresholds are poorer in older listeners than younger listeners across the frequency range, even at those typically considered unaffected by presbycusis. In the extended high frequencies typically not measured in the clinic (9-14 kHz), hearing thresholds in the older listeners drop precipitously. Although we characterize the speech range as 0.5-8 kHz, the extended high frequencies are also important for understanding speech, especially in noise.2
The Anderson et al. study investigated the factors contributing to age-related deficits in phase locking.1 Figure 2 shows significant decreases in phase-locking to the speech syllable /ba/ in older than younger listeners. We included audiometric and DPOAE thresholds and Wave I amplitude (representing auditory nerve function) in a model that predicted phase-locking strength. Given previous evidence of age-related synaptopathy,3,4 we hypothesized that Wave I amplitude, a proxy for synaptopathy, would contribute to the degradation of neural encoding at higher levels of the brainstem/midbrain. We found, instead, that DPOAE thresholds were the only factor that contributed to the strength of the phase locking. Therefore, even subtle declines in peripheral function may have consequences for the brain’s speech processing fidelity.

Overall, these results demonstrate the limitations of what we can conclude from a “clinically normal” audiogram. Even slightly elevated thresholds can affect central auditory dysfunction. This dysfunction is likely compounded by age-related changes in the brainstem/midbrain structures.5 It remains unknown how these deficits can best be managed. Investigations are ongoing to determine if low-gain hearing aids or auditory training can improve speech understanding in noise, especially in older listeners.
References
- Anderson S, Bieber R, Schloss A. Peripheral deficits and phase-locking declines in aging adults. Hear Res 2021;108188.
- Yeend I, Beach EF, Sharma M. Working memory and extended high-frequency hearing in adults: Diagnostic predictors of speech-in-noise perception. Ear Hear 2019;40:458–67.
- Parthasarathy A, Kujawa SG. Synaptopathy in the aging cochlea: Characterizing early-neural deficits in auditory temporal envelope processing. J Neurosci 2018;38:7108-7119.
- Sergeyenko Y, Lall K, Liberman MC, et al. Age-related cochlear synaptopathy: An early-onset contributor to auditory functional decline. J Neurosci 2013;33:13686-13694.
- Walton JP, Frisina RD, O’Neill WE. Age-related alteration in processing of temporal sound features in the auditory midbrain of the CBA mouse. J Neurosci 1998; 18, 2764-2776.