Something Important Requires Amplification in Clinical Audiology

Renowned auditory researcher Dr. Robert Harrison brings us up to date on information and research from the Labs. Appropriately titled “From the Labs to the Clinics”, Bob is involved in laboratory and applied/clinical research, including evoked potential and otoacoustic emission studies and behavioural studies of speech and language development in children with cochlear implants. For a little insight into Bob’s interests outside the lab and the clinic, we invite you to climb aboard Bob’s Garden Railway.
How best can I draw your interest to an important topic? Perhaps by saying that I am “frustrated, fed up, and completely saddened” by the lack of attention to it in clinical audiology. The topic is the cochlear mechanism that is singularly responsible for low threshold hearing and sound frequency analysis, and thus key to normal hearing. I refer, of course, to the cochlear amplifier.1–3
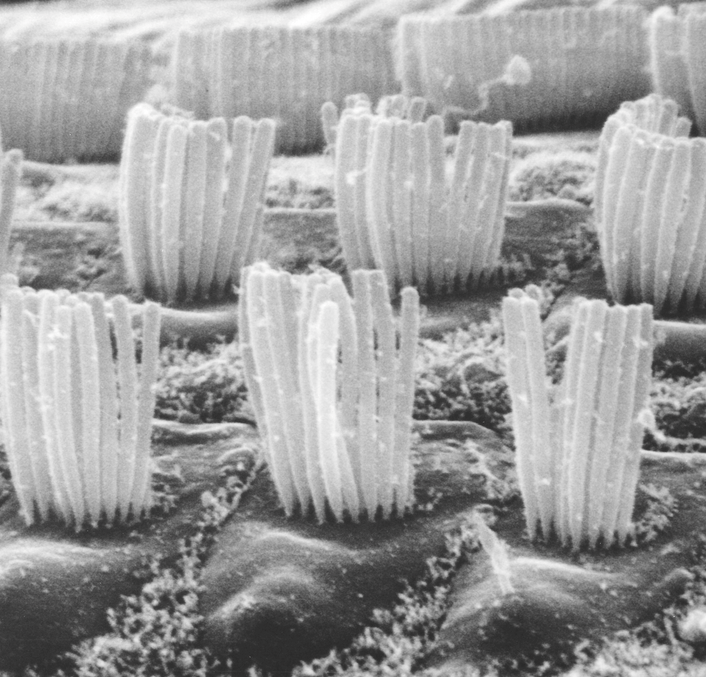
To remind you, this cochlear amplifier is an outer haircell mechanism that boosts up sound-driven mechanical movements within the organ of Corti and thus provides our exquisite sensitivity to low-level sounds. It also performs a frequency analysis and improves signal-to-noise ratio of signals detected by the inner haircells, and converted into a neural array of activity that the auditory brain can perceive and interpret.
For decades, hundreds (perhaps thousands) of researchers, including this author, have been studying and describing various aspects of the cochlear amplifier. Scientists have probed the active haircell mechanisms that can both detect and cause movement of the organ of Corti. Engineers have measured and modeled cochlear micro-mechanics. Physiologists have done controlled experiments to see the result of cochlear amplifier disruption. Genetics researchers have studied subjects with gene mutations that affect the cochlear amplifier. We have had almost a century of psychoacoustic research into auditory frequency analysis measures performed by the cochlear amplifier. Behavioural tests have been developed, including critical bandwidth measurement and psychophysical tuning curves. Objective electrophysiological measures have been proposed, including cochlear action potential tone on tone suppression curves.4–6

For some years, I have been writing in Canadian Audiologist about ideas and basic discoveries translating (or not) from the lab to clinics. On numerous occasions I have discussed various aspects of the all-important cochlear amplifier. From a clinical perspective, the cochlear amplifier is the key element of the inner ear function. Unfortunately, it is also a mechanism that is vulnerable to a wide range of insults, and when damaged, causes various types of hearing dysfunction. Almost all types of sensorineural hearing loss involve partial or total degradation of the cochlear amplifier, with just a few notable exceptions such as mild auditory neuropathy (SD), and inner haircell synaptopathy (hidden hearing loss).
In my last column in Canadian Audiologist I wrote about the “audiogram fine structure”. I emphasized that this test can reveal information about the cochlear amplifier. I also noted that another useful test, otoacoustic emissions, also probes the function of the cochlear amplifier. So, in addition to the behavioural and electrophysiological tests mentioned above, OAEs or audiogram fine structure can probe the integrity of the cochlear amplifier.
Why then are such tests not used clinically in audiology? Why is the most important mechanism of hearing ignored in clinical testing? I cannot understand; it is almost willful neglect!
If anyone is in disagreement with this opinion I urge you to respond. My email address is rvh@sickkids.ca. I would like to assemble your comments and report on them in my next column (assuming that I have not been dismissed by our editor in chief for heresy).
References
- Davis H. An active process in cochlear mechanics. Hear Res 1983;9:79–90.
- Dallos P and Evans BN. High-frequency motility of outer hair cells and the cochlear amplifier. Science 1995;267:2006–2009.
- Ashmore J. et al. The remarkable cochlear amplifier. Hear Res 2010;266:1–17.
- Harrison RV, Aran J.-M, and Erre J.-P. AP tuning curves from normal and pathological human and guinea pig cochleas. J Acoust Soc Am 1981;69:1374–85.
- Harrison RV and Aran J.-M. 1982. Electrocochleographic measures of frequency selectivity in human deafness. Br J Audiol 1982;16:179–88.
- Portmann M, Harrison RV, et al. Electrocochleographic measures of cochlear frequency selectivity in hearing loss of cochlear origin. Acta-Otolaryngol 1983;95:657–63.