Engaging and Empowering Children and Adolescents Using Connected Hearing Healthcare

![]() The digital revolution has enabled the potential to leverage technological innovation, bringing the reality of “connected health” to patients and stakeholders involved in the care process. Connected health is best described as a model of healthcare delivery that is focused on people, processes, and technology. The connected health model encompasses terms such as mobile (mHealth), electronic (eHealth) and tele (tele-health) and involves devices, services, or interventions designed around the patient's needs; it can enable proactive and efficient sharing of health-related data.1 In hearing healthcare, a connected model brings the potential to offer patient-centered audiological services at a distance using exciting new hearing device technology. As technology and connectivity continue to evolve so can the audiological care process, by capitalizing on hearing healthcare technology advances, optimizing service delivery access and sustainability, and empowering the patient in the care process. Tele/virtual appointments are now possible via connected technologies, allowing for improved access to services in both rural and urban communities.
The digital revolution has enabled the potential to leverage technological innovation, bringing the reality of “connected health” to patients and stakeholders involved in the care process. Connected health is best described as a model of healthcare delivery that is focused on people, processes, and technology. The connected health model encompasses terms such as mobile (mHealth), electronic (eHealth) and tele (tele-health) and involves devices, services, or interventions designed around the patient's needs; it can enable proactive and efficient sharing of health-related data.1 In hearing healthcare, a connected model brings the potential to offer patient-centered audiological services at a distance using exciting new hearing device technology. As technology and connectivity continue to evolve so can the audiological care process, by capitalizing on hearing healthcare technology advances, optimizing service delivery access and sustainability, and empowering the patient in the care process. Tele/virtual appointments are now possible via connected technologies, allowing for improved access to services in both rural and urban communities.
The connected hearing healthcare (CHHC) delivery model can be applied to many audiological services, however, recent research efforts have largely focused on the use of mobile devices and related applications to support patients in their aural (re)habilitation journey. Applications (aka, apps) on mobile devices are allowing us to learn more about patients’ real-world experiences, challenges, and listening performance. Apps can be classified in 4 domains: (1) screening and assessment, (2) intervention and rehabilitation, (3) education and information, and (4) assistive tools.2 Screening and assessment apps present a unique opportunity to gather rapid self-report data related to patients’ daily life experiences via survey-based methods. This information can now be linked to the performance of the hearing aid via Bluetooth connection between devices, or manually by the user. Mobile-based ecological momentary assessment (EMA) is often used in research to collect participants’ data in real-time and real-world contexts. EMA aims to minimize recall bias, maximize ecological validity, and allow the study of microprocesses that influence behavior in natural environments.3 A growing number of studies, including adult participants, report EMA as a feasible and valid research method for use with hearing-impaired listeners.4–6
When it comes to the digital revolution, technological advances are largely experienced and enjoyed by children and youth. Commonly referred to as “digital natives” are today’s young people who were born into the digital era, growing up exposed to the continuous flow of digital information and technologies, and for whom computers and the Internet are natural components of their lives.7 It seems reasonable to assume that connected technologies may help engage children and adolescents while offering the many benefits experienced by adult users. However, further research is needed to realize the benefit of a CHHC model of care with younger populations. A CHHC model has the potential to “connect” children and adolescents via technology to the stakeholders involved in their hearing healthcare journey and as part of their daily life experiences. This potential is illustrated in Figure 1.
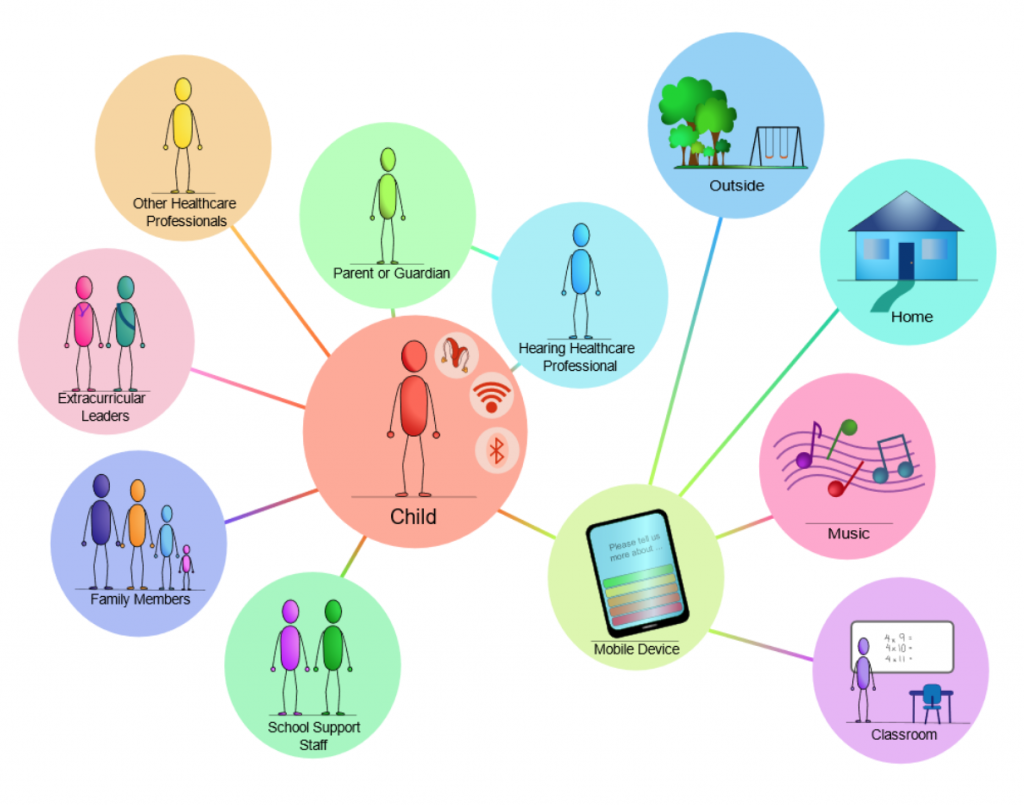
Figure 1. Illustration of the potential for technology to connect children and adolescents with hearing impairment to important stakeholders using data-driven processes.
A recent study by Gwen Carr suggests that distance technology, such as remote hearing aid fitting, may help re-engage and empower adolescents to have greater ownership and positive management of their hearing needs.8 When considering mobile app research, studies from the general health literature are contributing to a growing body of evidence around the use of mobile-EMA methodologies with children and adolescents. Included in a systematic review of this literature is the use of EMA to assess behaviors, subjective experiences, and contextual information; moderate compliance rates are reported among these EMA studies included, largely thought to be influenced by factors including the type of sampling, the time and frequency with which EMA data is sampled, and the age of the participants.9
A recent study from Western University's National Centre for Audiology looked at the use of EMA with children and adolescents wearing hearing aids to learn about preference for and performance with a prescription-based noise management strategy in real-world contexts. The study design included the recruitment of older children, the use of minimal event-based sampling over a week-long trial, and child-initiated prompts outside of school time (Figure 2). Event-based sampling allowed the children to engage in EMA when in listening situations of interest that presented challenging and non-challenging hearing scenarios.
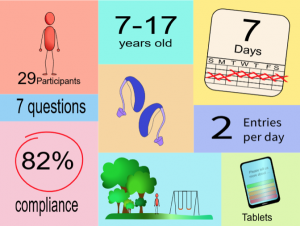
Figure 2. A summary of the study design factor contributing to good compliance among child and adolescent hearing aid users, in a real-world EMA study.
For this study, compliance was slightly higher for the younger group (< 12 years of age), compared to the adolescent group. One factor that may have contributed to this finding was the greater presence of parental involvement among the younger group. As we continue to learn from this study, some clear points have emerged.
- EMA is a feasible research method with children and adolescent participants and high compliance rates can be obtained in studies with minimal participant burden.
- Participants could easily complete ratings of noise and speech understanding, answer multiple-choice questions, and offer preference-based survey responses, accessed through an app on a tablet.
- EMA was completed during daily listening activities, which allowed for the collection of in-the-moment and contextual self-report data linked to hearing aid performance.
- Although the children could easily use manual program switching, further EMA research employing Bluetooth pairing and automatic switching may eliminate this need.
- The children and adolescents reported experiencing a high proportion of noisy listening environments outside of school time, reinforcing the need for aided noise management strategies with children and adolescents.
- A prescription-based noise management strategy (based on DSL v5.0 child) may help reduce loudness for children and adolescents in noisy situations.
- A high level of enthusiasm was observed around the use of connected technologies and around the children and adolescents’ being able to contribute to their own hearing aid fitting experience; parental involvement in EMA was observed with some of the younger participants.
Although further research is needed to fully incorporate a CHHC model of care into the aural (re)habilitation process for children and adolescents, this model of care has the potential to offer many benefits. Along with improved accessibility to services via tele/virtual models of delivery, technology-enabled hearing healthcare offers the potential to engage and empower the user; this may be especially important in the care process for children and adolescents. As the hearing experience for children is dynamic, so should their care process be. Research informing the design of connected technologies should involve the end-user and all stakeholders, at all levels. Successful implementation of CHHC will rely on studies to demonstrate its benefit to the end-user and an overall better understanding of the factors involved in the implementation process. And last but not least, the CHHC model of delivery relies on knowledge creation and dissemination around the maintenance of patient confidentiality and privacy during all processes.
Acknowledgments
The research presented in this article has been supported by the Ontario Research Fund (ORF RE08-072) and by licensing revenues from technology transfer and was made possible through collaboration with my colleagues Drs. Susan Scollie and Maaike Van Eeckhoutte. The devices used in the study were donated by Phonak AG, along with the software tools to enable the mobile-based survey.
References
- Caulfield BM and Donnelly SC. What is connected health and why will it change your practice? QJM 2013;106(8):703–707. https://doi.org/10.1093/qjmed/hct114
- Paglialonga A, Tognola G, and Pinciroli F. Apps for hearing science and care. Am J Audiol 2015;24(3):293–98. https://doi.org/10.1044/2015_AJA-14-0093
- Shiffman S, Stone A, and Hufford MR. Ecological momentary assessment. Ann Rev Clin Psychol 2008;4(1):1–32. https://doi.org/10.1146/annurev.clinpsy.3.022806.091415
- Timmer BHB, Hickson L and Launer S. Ecological momentary assessment: Feasibility, construct validity, and future applications. Am J Audiol 2017;26(3S):436–42. https://doi.org/10.1044/2017_AJA-16-0126
- Timmer BHB, Hickson L, and Launer S. The use of ecological momentary assessment in hearing research and future clinical applications. Hear Res 2018;369:24–28. https://doi.org/10.1016/j.heares.2018.06.012
- Wu YH, Stangl E, Zhang X, and Bentler RA. Construct validity of the ecological momentary assessment in audiology research. J Am Acad Audiol 2015;26(March 2015):872–84. https://doi.org/10.3766/jaaa.15034
- Dingli A and Seychell D. The New Digital Natives. Springer Berlin Heidelberg; 2015 https://doi.org/10.1007/978-3-662-46590-5
- Carr G. Using telehealth to engage teenagers. ENT Audiol News 2017;25(6):1–2.
- Wen CKF, Schneider S, Stone AA, and Spruijt-Metz D. Compliance with mobile ecological momentary assessment protocols in children and adolescents: A systematic review and meta-analysis. J Med Internet Res 2017;19(4 e132):1–14. https://doi.org/10.2196/jmir.6641