Hearing Aid Candidacy for Children with Mild Bilateral Hearing Loss

![]() Children with hearing loss have greater developmental potential than ever before thanks to universal newborn hearing screening and early diagnosis, amplification, and early intervention. Even with these advances, children with mild bilateral hearing loss can be at risk to miss out on the benefits of early intervention and amplification because of clinical equipoise among audiologists. Clinical equipoise refers to a situation where professional disagreement exists about the appropriate course of action due to a lack of scientific consensus regarding an intervention. The decision about whether children with mild bilateral hearing loss can benefit from early identification and intervention remains controversial,1 despite emerging evidence that children with mild bilateral hearing loss who receive amplification and intervention have stronger skills in some areas of language than peers who do not receive these interventions.2 Practicing audiologists are often caught between these opposing views without clear guidance on whether to provide amplification for children with milder degrees of hearing loss.
Children with hearing loss have greater developmental potential than ever before thanks to universal newborn hearing screening and early diagnosis, amplification, and early intervention. Even with these advances, children with mild bilateral hearing loss can be at risk to miss out on the benefits of early intervention and amplification because of clinical equipoise among audiologists. Clinical equipoise refers to a situation where professional disagreement exists about the appropriate course of action due to a lack of scientific consensus regarding an intervention. The decision about whether children with mild bilateral hearing loss can benefit from early identification and intervention remains controversial,1 despite emerging evidence that children with mild bilateral hearing loss who receive amplification and intervention have stronger skills in some areas of language than peers who do not receive these interventions.2 Practicing audiologists are often caught between these opposing views without clear guidance on whether to provide amplification for children with milder degrees of hearing loss.
Uncertainty about whether to provide amplification for children with mild bilateral hearing loss is apparent from several recent studies. Fitzpatrick and colleagues showed that children with mild bilateral hearing loss were less likely to receive amplification than peers with greater degrees of hearing loss. Children with mild bilateral hearing loss who did receive hearing aids were not fitted until 9 months of age on average.3 Similarly, the aforementioned study by Walker et al.2 showed inconsistency in whether children with better-ear pure tone averages (PTA) less than 30 dB were fitted with hearing aids. These results suggest that audiologists may have some uncertainty about whether to fit hearing aids and the timing of hearing aid fitting for children with mild bilateral hearing losses. This may be particularly true for infants who are diagnosed with mild bilateral hearing loss using auditory brainstem response, where the minimum test levels are often a range that makes it challenging to differentiate mild hearing loss and normal hearing levels.
To provide an additional tool for hearing aid candidacy for children with mild bilateral hearing losses, our research team examined audiological and language data for a group of children that were followed longitudinally as part of the Outcomes of Children with Hearing Loss study.4 In the cohort for the study, there was a subgroup of children with varying degrees of hearing loss who did not receive or did not consistently use hearing aids. A relatively large group of children who did not receive or use amplification presented an opportunity to examine the relationship between unaided hearing and language outcomes. Figure 1 shows data adapted from McCreery and colleagues that shows the relationship between unaided hearing (the Speech Intelligibility Index; SII) and language scores.5 The unaided SII estimates the weighted proportion of speech that is audible to a listener for average speech when a talker is one meter away based on their audiogram and ear canal acoustics. For children with unaided SII below 80 (green line in Figure 1), language scores increased as audibility increase. For children with unaided SII greater than 80, increases in audibility did not lead to a significant improvement in language scores (blue line in Figure 1), potentially because those children had language scores that were within the range of children with normal hearing.
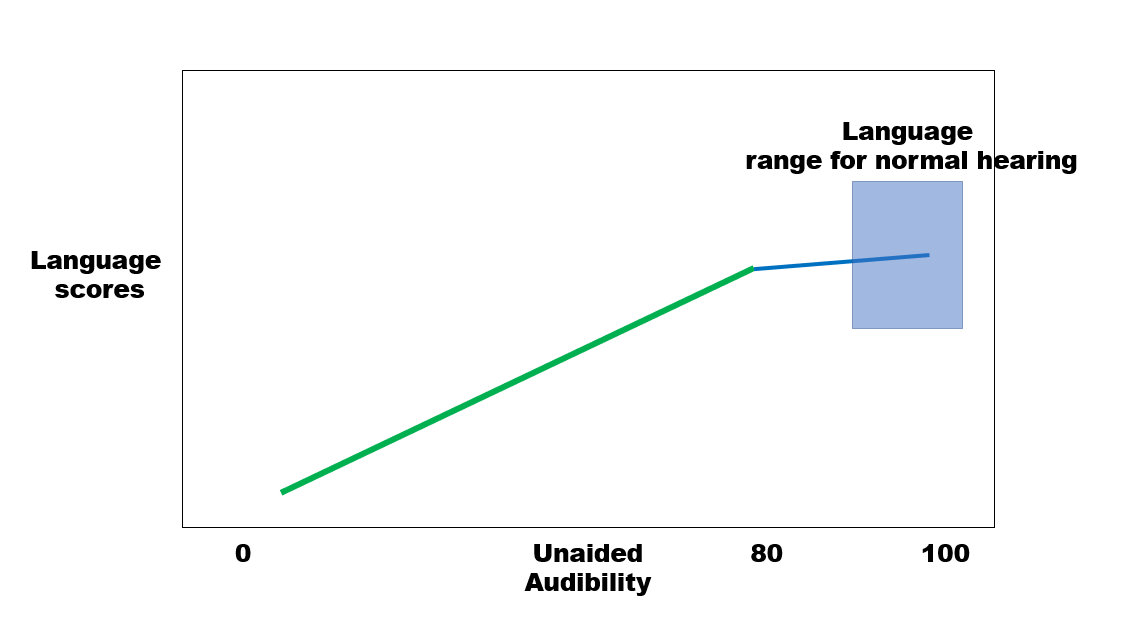
Figure 1. Language scores plotted as a function of unaided audibility for speech for children who did not receive or use hearing aids (adapted from McCreery et al. 2020).5 The green line represents the linear relationship between language and unaided audibility for the portion of the range where increasing audibility is associated with increasing language outcomes. Around an unaided audibility level of 80, the benefit of improving audibility on language scores is reduced as depicted by the blue line. The blue shaded box represents the average range of language scores for children with normal hearing. This pattern was observed across three different language outcomes.
The main clinical implications of these findings are that the unaided SII can be used to assess hearing aid candidacy for children with hearing loss. The dB HL audiogram does not reflect the effects of ear canal acoustics and hearing levels on speech audibility, particularly for insert earphones. Clinicians can use hearing aid verification systems to simulate (using an age-related average real-ear-to-coupler difference; RECD) or measure (using a measured RECD) unaided SII for a given hearing loss. Children with unaided SII less than 80 should be considered candidates for hearing aids, whereas children with unaided SII greater than 80 should have their hearing and speech and language skills monitored periodically, as some recent estimates suggest that nearly 50% of children who initially present with mild degrees of hearing loss may eventually progress to greater degrees of hearing loss.6
Some caveats should be considered when applying this approach clinically. Some children with unaided SII greater than 80 had language scores that were significantly poorer than peers with normal hearing. Thus, some children may be candidates for hearing aids even if their unaided audibility is greater than 80. The unaided SII criterion is a more informative element to hearing aid candidacy decisions than the dB HL audiogram, but it is not a replacement for the numerous other factors that audiologists consider when making decisions about amplification for infants and young children. This approach should also be validated prospectively with a new cohort of children with hearing loss to demonstrate that the results observed in this study replicate and generalize as anticipated.
References
- Carew P, Mensah FK, Rance G, et al. Mild–moderate congenital hearing loss: Secular trends in outcomes across four systems of detection. Child: Care Health Development 2018;44(1):71–82.
- Walker EA, Holte L, McCreery RW, et al. The influence of hearing aid use on outcomes of children with mild hearing loss. J Speech Language Hear Res 2015;58(5):1611–25.
- Fitzpatrick EM, Whittingham J, and Durieux-Smith A. Mild bilateral and unilateral hearing loss in childhood: A 20-year view of hearing characteristics, and audiologic practices before and after newborn hearing screening. Ear Hearing 2014;35(1):10–18.
- Moeller MP and Tomblin JB. Epilogue: Conclusions and implications for research and practice. Ear Hearing 2015;36(0 1):92S.
- McCreery RW, Walker EA, Stiles DJ, et al. Audibility-based hearing aid fitting criteria for children with mild bilateral hearing loss. Language, Speech, and Hearing Services in Schools 2020; 51(1), 55-67.
- Fitzpatrick EM, Nassrallah F, Vos B, et al. Progressive hearing loss in children with mild bilateral hearing loss. Language Speech Hear Services Schools 2020;51(1):5–16.