Remote Teleprogramming of Hearing Aids

Introduction
Hearing aids have improved substantially over the years. In spite of this, no hearing aid has been able to provide a complete substitute for one’s original hearing. Even though thousands of practical electroacoustical programming possibilities are available in current hearing aids, what is not controlled are the non-specific subjective expectations of the hearing-impaired patient. And, it is these that are most likely to determine the final element to successful use, even more so than any electroacoustical improvements.
It is recognized that what sounds subjectively acceptable in different listening environments differs among individuals. Because of this, it is reasonable to expect that different listening strategies for acceptable amplification may be required. With current hearing aids, the chip circuit consists of a single hearing aid in which its parameters can be changed extensively by adjustments via the programming device. The instrument remains, however, the same hearing aid – its basic architecture has not changed. Within this architecture, adjusts of the parameters are made either through a formula selection and/or then employing a non-specific “fit and modify” approach to hearing aid selection, all made using a programming device (PC with proprierary software from a given hearing aid manufacurer) in the fitter’s office. Such adjustments are made until the patient is either satisfied, or led to believe that the fitting is the best that can be provided at the time, and the patient must learn to accept the amplification being received. Often, after the patient stops complaining or returning for adjustments, is the designation made that the fitting has become “acceptable.” In many cases, hearing aid manufacturers have made available hand-held remote controls that change the hearing aid’s gain and response options that provide some user control of the signal. However, the remote controls are not used to reprogram the hearing aid.
In the late 1970s, a system was introduced that allowed the patient to access different hearing aid performance strategies and meet subjective needs via a hand-held remote control, but also allowed the system to be reprogrammed remotely (outside the dispenser’s office). This application was called remote teleprogramming (RTP).
The Mechanics
In 1997, Philips (what was then the Philips Hearing Instruments Company), developed a remote teleprogramming (RTP) approach to hearing instrument performance selection that expanded the patient’s subjective sound preference by allowing the system to be reprogrammed as a completely different hearing aid, not just to set and store parameter changes.1 The interesting feature of this system was that the reprogramming could be accomplished without requiring face-to-face contact between the dispenser and patient. The reprogramming could be performed remotely. In essence, the multi-programmer remote contained its own programmable memory, with the changes passed on to the worn device. In this case, via infrared. In reality, the multi-programmer was the hearing aid, and the device worn at ear level was primarily the transmission system. So, what this provided was the ability to reprogram the hearing aid, not to just provide a remote control or Smart Phone app that the patient could use to make primarily gain, response, and environmental listening selections.
This post describes briefly the mechanics of the system, suggesting that the “low-technology” used then, could still be employed, especially if someone chose not to go the “high-tech” route using the Internet.
As the title implies, the reprogramming was/can be performed via the telephone, literally from anywhere in the world. The system provided a practical, and simple application to the information highway without the need for Bluetooth connections, pairings, and sophisticated computer devices. At the user’s end (Figure 1), the system consisted of a hearing aid and a hand-held remote control (multi-programmer).
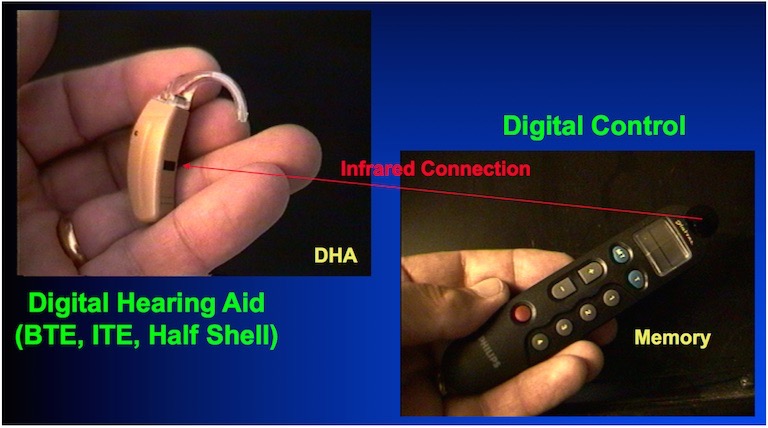
Figure 1. Hearing aid system, consisting of a hearing aid (left) and a user controlled hand-held remote multiprogrammer (right).
In the way the system was presented, the hearing aid received patient commands from the hand-held multi-programmer, in this case, via infrared, acting as a conventional hand-held remote control. But, communication between the two devices could be by other means, with the multi-programmer memory being the heart of the system. It allowed for a number of programs that could be set by the dispenser through four different methods:
- As a stand-alone programming tool
- By a personal computer that would transmit the programming through close proximity acoustic coupling (using the computer’s internal speakers, although external speakers were preferred),
- By remote teleprogramming reception via telephones that use DTMF signals (Figure 2), and
- By the use of a telephone interface device, similar in design to the remote multi-programmer. This was a non-user remote, but which had a telephone symbol and three small opening to indicate where the acoustic coupling occurred.
Option #3, the fact that the system could be reprogrammed from the patient’s own listening environment, and from anywhere in the world, was the first time such an option had been available for hearing aids. In essence, it extended the remote control as a computer, rather than a passive device to allow for pre-programmed adjustments. Figure 2 shows the reprogramming as it moves along the information highway.
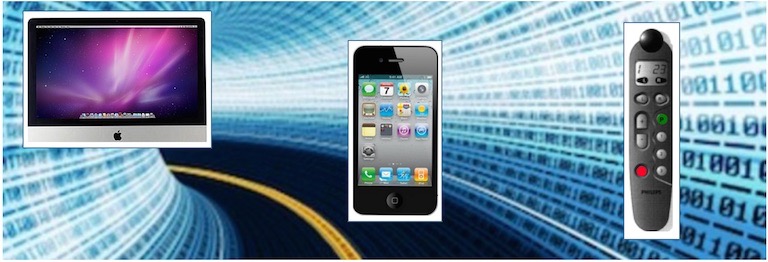
Figure 2. Remote teleprogramming (RTP) allows for hearing aid acoustical performance to be modified via the telephone from anywhere in the world. The telephone (center) is acoustically connected to the multi-programmer remote control (right). The telephone receives its DTMF signals from the primary computer program (left).
Remote Teleprogramming (RTP)
To reprogram the system remotely, the multi-programmer (hand-held remote control) was acoustically coupled to a telephone (physically held against the telephone receiver for activation). The ability to transmit information acoustically over the telephone was based on the use of DTMF (Dual Tone Multi-Frequency) technology that used audio tones to send telephone signals (i.e., the beeps heard during dialing). The basic concept of DTMF is that two frequency-specific output tones in the voice band are combined to represent a number. Without going into since-added options, the dual tone method produced 12 unique combinations from only seven tones – the frequencies of which have been internationally standardized (providing the opportunity to reprogram a hearing aid from anywhere in the world). When incorporated into integrated circuitry, the DTMF-generated tones provided codes that corresponded to information transmitted according to proprietary algorithms. The receiving unit (in this case the hand-held remote control) filtered and decoded these tone sequences picked up acoustically from the telephone receiver. The performance of the decentralized programmable memory of the system was then modified accordingly.
Validation of the transmitted algorithm in the DTMF receiver required that the transmitted signal code be received twice (with exactness) to access changes. This allowed for greater cost control through timely, shorter and/or fewer office visits.
Is DTMF Technology Still Applicable?
Yes. In fact the world would not operate well without DTMF use. It is used to transmit signals over a radio, turn items on and off, flash lights, control motors, cameras, activate warning systems, turn on irrigation systems, open gates, and in general, control the world.2 The DTMF signal was originally decoded by tuned filter banks, but digital signal processing is now the predominant technology for decoding.
“Why not use computer signals instead of DTMF? Radio frequency controlled devices are often designed by engineers to operate in the normal human voice range. This means that DTMF passes transparently over normal two-way radio channels, narrow-band or wide-band. It doesn’t require special channel widths, or expensive equipment. In most instances you can simply attach a cable to the speaker output of a two-way radio to a decoder, and it will be ready to go. It’s straighforward, fast, easy to understand, works on most any type of radio, and gives the most flexible features for the lowest cost!”
References
- Staab W, Edmonds J, Garcia H. Remote teleprogramming (RTP): future directions to patient management. High Perform Hear Solut 1977;2:50–52.
- Genave Electronics. Genave explained. Rosemount, MN, Author. Available at: http://www.genave.com/dtmf.htm.