Industry Research – Fine-Tuning Outcomes are Similar via Teleaudiology and Face-to-Face

Telehealth comprises ways to enhance the provision of health care, education and support using telecommunications technologies, and is increasingly a component of the care provided by healthcare professionals. As in other health related fields, teleaudiology has the potential to enhance care and meet expectations of patients in audiology clinical practice, but has not yet been widely embraced. Discussion of the benefits of teleaudiology has focused on the improved access to care for persons who have difficulty coming to appointments due to distance or other constraints. However, the benefits are not limited to overcoming this issue or even to patients, as there are also significant potential wins for hearing care professionals (HCPs) and business practices.1 For example, cost and workflow efficiencies can be of benefit to practices, HCPs and patients. In an analysis of the appointments of a large hearing aid dispensing practice over a 9-year period, it was found that appointments for fine-tuning were the most frequent, with 28% of total appoints being for this purpose. Furthermore, the actual contact time for fine-tuning appoints is brief, with 96% lasting less than 30 minutes.2 However, consider that the actual time used by the HCP, practice staff, and client to make the appointment happen goes far beyond 30 minutes, and it becomes obvious how teleaudiology might reduce costs and increase efficiency for all parties.
As in many industries, cloud-based services are being introduced in the hearing aid industry. One application of such services is to support communication between the HCP and the hearing aid user. ReSound Assist is a teleaudiology tool that enables hearing aid users to request assistance from their HCP via the ReSound Smart 3D app on their personal smart device.3 The HCP can respond with a message, but can also make adjustments to the fitting and send these adjustments back to the user as an update. The user can then transfer this update to their hearing aids via the wireless connection between the smart device and the hearing aids. This application requires relatively little investment for the HCP and user in terms of equipment and infrastructure. Because it does not require a live interaction where both the HCP and user must be present at the same time, it also offers a high degree of flexibility for a practice to implement.
An initial question that must be answered before adopting any teleaudiology practice is whether the effectiveness of providing the service in this way matches the quality of the service provided in person.4 To that end, an investigation was carried out to compare objective and subjective outcomes when performing fine-tuning of hearing aid fittings in a traditional face-to-face interaction versus fine-tuning using Resound Assist. Because tools intended to improve outcomes or facilitate processes can themselves be barriers, usability and user perception of ReSound Assist were also evaluated.
Methods
Participants
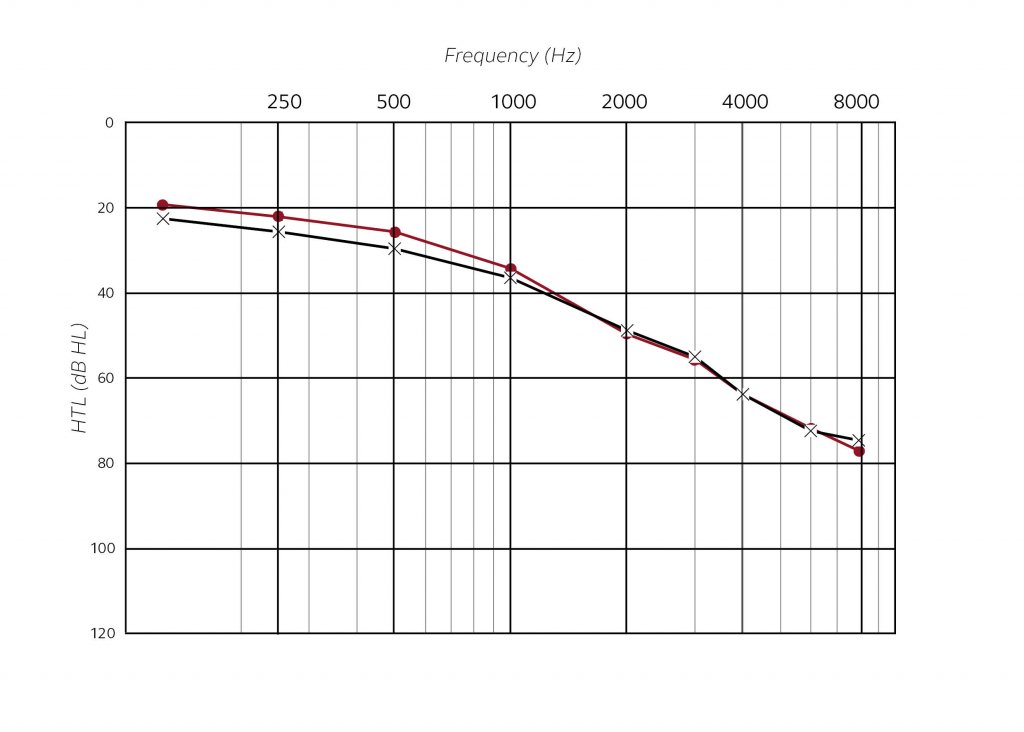
Fourteen adult hearing aid users ranging in age from 58 to 79 years (mean 67.1 years) participated in this study. There were 11 men and 3 women. The mean hearing threshold levels of the participants are shown in Figure 1. All owned and used smartphones. Ten of the participants owned smartphones that were compatible with the ReSound Smart 3D app.
Technology readiness
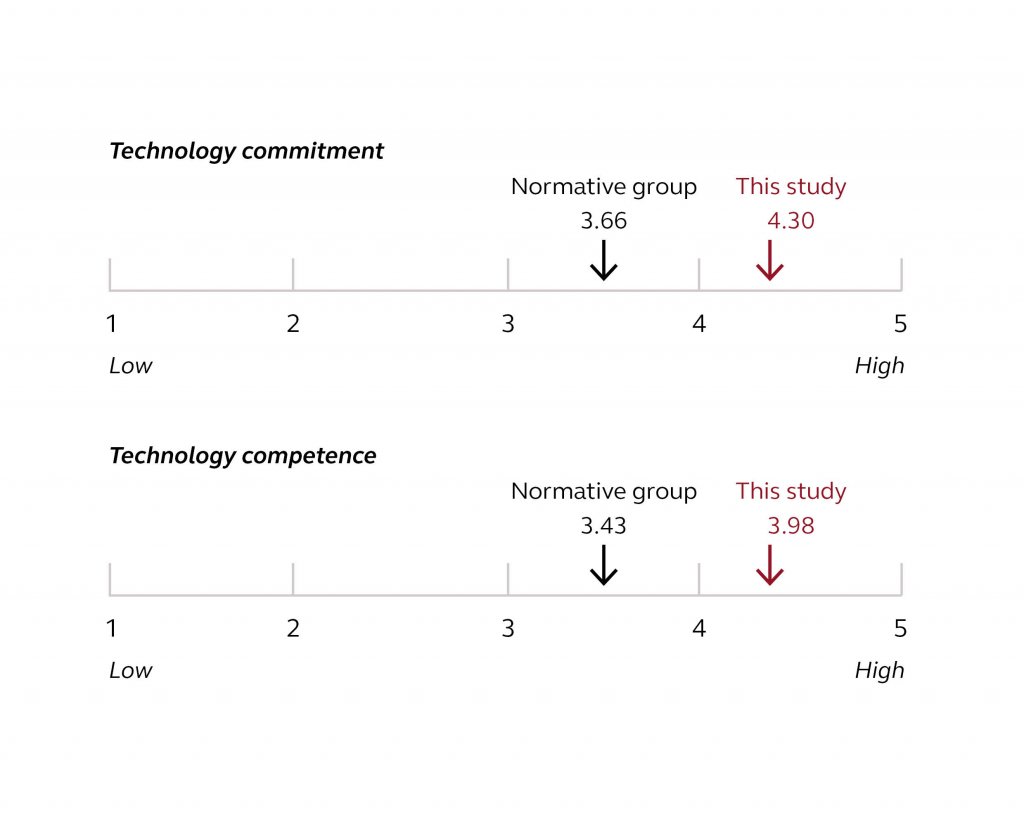
One selection criterion for participants in this study is that they were smartphone owners. Although smart device ownership among older adults who make up the majority of hearing aid users is increasing, this was nevertheless a potential source of bias in the study that could limit the application of the results. Therefore, we sought to qualify how “tech savvy” the participants in the study were compared to others in their age group. Neyer et al5 proposed a model of technology commitment to predict the adaptive use of technology, especially among older individuals. There are three facets to the model: technology acceptance, technology competence and technology control. The participants’ overall technology commitment was evaluated per this tool. The results of the technology commitment (total scale) and technology competence sub-scale were compared with results from a representative population that included 748 males from 55 to 79 years of age6, which is similar to the age range of our study participants, most of whom were men. Our participants showed higher technology commitment and technology competence than their age cohorts by about at least one-half scaling unit.
Procedures
Participants attended four sessions. At the first session, they were bilaterally fitted by the HCP face-to-face with ReSound LiNX 3D 962 RIE hearing aids with one program set to manufacturer defaults for quiet situations. No fine-tuning was done at the initial fitting. The Göttingen sentence test (GÖSA)7 was administered to determine the Signal-to-Noise Ratio (SNR) for 50% correct with the hearing aids. Real ear measurements were made to document the fitted responses and participants were sent out to a daily life test for one week. Participants were given a questionnaire to return at the next visit based on their experience with the hearing aids during the week. The questionnaire included the International Outcome Inventory for Hearing Aids (IOI-HA)8 along with questions taken from two other questionnaires to supplement the global assessment of the IOI-HA with more information regarding hearing benefit and listening effort. To that end, five questions from the Speech, Spatial and Qualities of Hearing Scale9 were added to provide information regarding hearing benefit. Two questions were from the pragmatic subscale of multiple speech streams and the remaining three addressed speech in noise, identification of sound, and localization. Three additional questions from the German Listening Effort Questionnaire10,11 were added to provide a subjective assessment of listening effort.
After one week, participants returned for the second visit. The participants were randomly assigned to one of two groups for fine-tuning. Fine-tuning was performed by adding and adjusting a second program intended for listening in noise using a laboratory noise situation to elicit fine tuning needs. Group A (seven participants) interacted in person with the HCP, and the HCP made the fine-tuning adjustments. Video recordings of the fine-tuning sessions were recorded for off-line analysis of the dialogue between the HCP and the participant. First, adjustments to the noise listening program were made based on the individual’s feedback in the noisy laboratory listening situation, thereafter addition adjustments to the quiet situation program were made based on the individual’s experience during the week of wear time. This condition represents how hearing aids typically would be adjusted by the HCP in an in-person encounter.
The second group of seven individuals, Group B, was given a basic orientation to use of the ReSound Smart 3D app and the ReSound Assist feature. They were shown to a separate room from the HCP, where they used ReSound Assist to request fine-tuning changes to both of the hearing aid programs beginning with the program for listening in noise situations and followed by the first program (they first had the opportunity to listen to the noise program in the noisy laboratory environment prior to using ReSound Assist). All participants were retested with the GÖSA for both hearing aid programs and the hearing aid responses were documented with real ear measurements. After using ReSound Assist, Group B participants completed a German version of the System Usability Scale (SUS).12 This scale gives a global subjective assessment of usability and is administered before any discussion or debriefing takes place, thereby reflecting the users’ immediate experience with the system. All participants in both groups were also given the same questionnaire as at the first session to fill out at home prior to the next visit.
After 2 weeks of hearing aid wearing time in their daily environments, participants returned for the third session. The fine-tuning method was switched across groups. The group who had used ReSound Assist for fine-tuning met with the HCP for face-to-face fine-tuning based on any issues in daily use, while the group who had previously had fine-tuning done in person used ReSound Assist to request necessary fine-tuning. Retesting with the GÖSA and real ear measurements were carried out, and the group who used ReSound Assist for fine-tuning filled out the SUS usability questionnaire.
Finally, the 10 participants who owned smartphones that were compatible with the ReSound Smart 3D app wore the hearing aids for an additional four weeks. These participants were encouraged to use ReSound Assist during the remainder of the trial period to request further fine-tuning if needed. They also completed the questionnaire prior to the concluding visit.
Results and discussion
The primary research question of this study was whether fine-tuning outcomes using ReSound Assist were comparable to outcomes when fine-tuning was done in person. This was assessed by the speech recognition testing, subjective assessment via the questionnaire, and real ear measurements. Other research goals were to assess the usability of ReSound Assist, compare the communication structures that inform the fine-tuning process for each method, and to uncover preferences, advantages and disadvantages of the two methods from the users’ perspective.
Speech recognition
Participants received fine-tuning for the first time at visit 2. Fine-tuning was done both for the newly added program for listening in noise (P2) and for the default listening program (P1). The average GÖSA results were not significantly different after fine-tuning of P1 regardless of whether fine-tuning was done face-to-face or remotely via ReSound Assist. In addition, speech recognition in noise was better for P2 than for P1 and the average magnitude of the improvement with P2 was approximately 1 dB regardless of the fine-tuning approach. Results were similar at the third visit, where the method for fine-tuning was switched between the groups. No significant differences were observed after fine-tuning compared to baseline for either group.
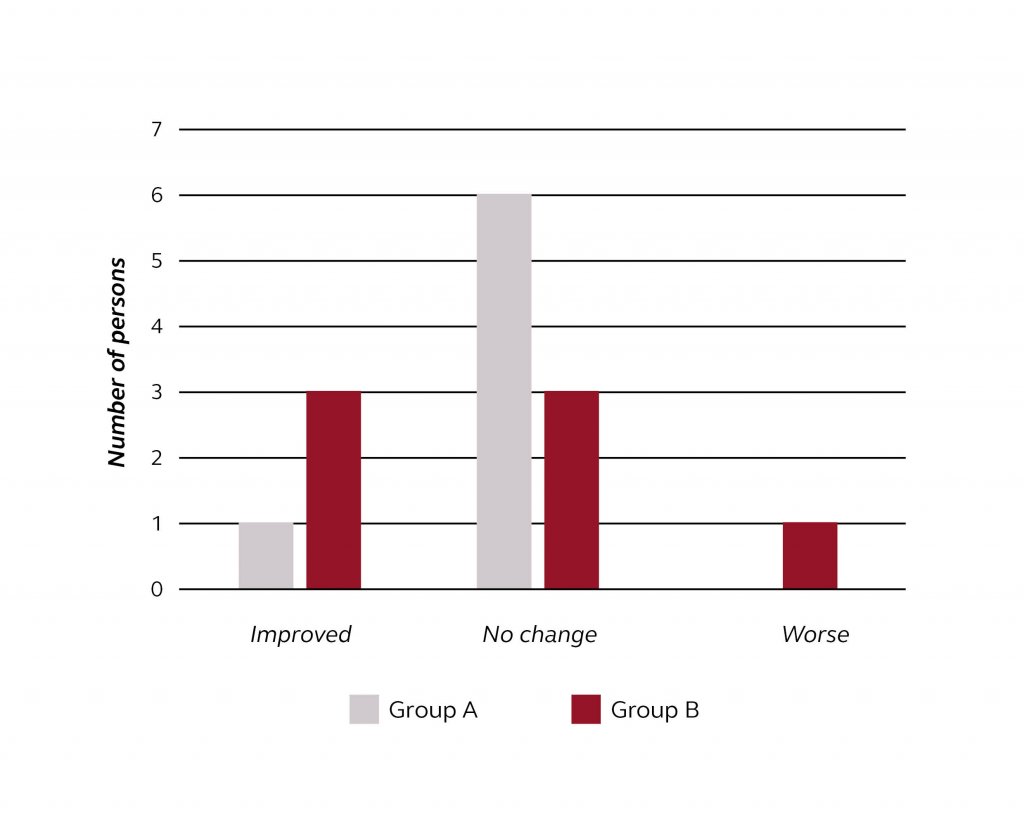
The main hypothesis in this study was that the method used for fine-tuning would not be related to differences in outcomes. Looking at averaged results, this hypothesis is supported for speech recognition in noise. However, it is also of interest to examine whether individuals might be impacted differently than is reflected in the averaged results, as this is really the most interesting question for the HCP. In other words, can we anticipate that some individuals may do much better or worse with one method or the other? Figure 3 shows how many individuals improved, showed no change, or did worse on the speech recognition task in P1 for each of the experimental groups. For this purpose, an individual score difference of 2 dB is considered a clinically meaningful difference in performance. One individual showed a decrease in performance at the final evaluation relative to baseline. This person was in Group B, who were the ones that were fine-tuned via ReSound Assist at visit 2, and face-to-face at visit 3. While the sample size of this study is not large enough to draw definitive conclusions, it does not appear that individuals are harmed by starting with one fine-tuning method versus the other. However, it should be considered that the participants in the current study showed a higher level of technology competence and commitment than a normative group.
While this finding does not point to the superiority of one fine-tuning method over the other, it could have implications for an optimized protocol with a remote fine-tuning tool. It could be that an initial face-to-face interaction lays the groundwork for a common understanding of how to describe hearing aid sound experiences, and that this positively impacts effective use of the remote method. Using ReSound Assist in this manner would be consistent with common clinical practice, where hearing aids are professionally fit, and the initial follow-up is done at an in-person appointment.
Subjective outcomes
The change in responses from baseline to the third session on the IOI-HA did not differ between the group that was initially fine-tuned face-to-face and the group that used ReSound Assist for the initial fine-tuning. For the 10 participants who owned a compatible smartphone and who wore the hearing aids an additional 4 weeks with access to ReSound Assist, their final responses were not significantly different than the baseline, which was the responses collected during the first trial week. The average responses trended marginally lower than baseline, but this is consistent with findings in longitudinal investigations of subjective outcomes with hearing aids where subjective outcomes may decrease slightly over time.13,14 Results were similar for the supplementary questions on hearing benefit and listening effort. No differences were detected between the two groups from baseline to session 3, and no significant differences were observed from baseline for the 10 participants who used the hearing aids an additional 4 weeks and could use ReSound Assist during this time. Similar to the speech recognition results, these findings are encouraging, as they support that users do not perceive varying benefit based on the method of fine-tuning.
Real ear measurements
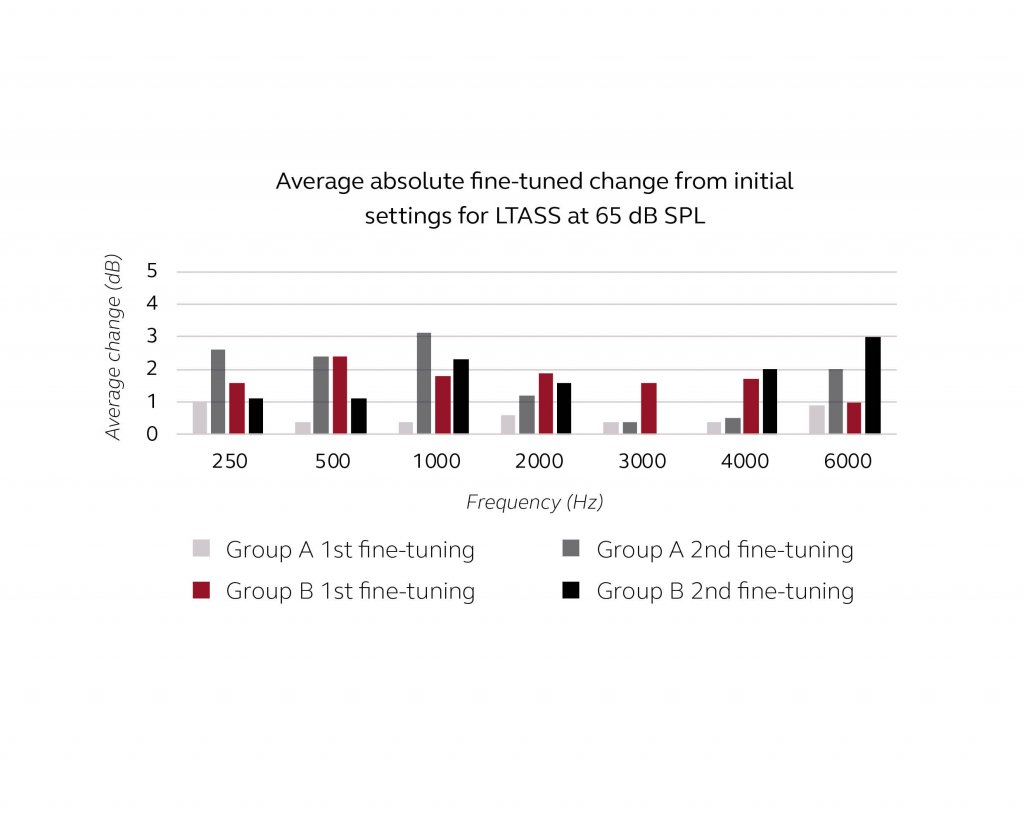
Figure 4 shows the average fine-tuned changes at the first and second fine-tunings relative to the settings of program 1 (P1) at the initial fitting. Only the results for the LTASS at 65 dB SPL are presented, as the percentile analysis showed similar patterns for the ninety-ninth and thirtieth percentiles. This suggests that changes were mostly made to the overall frequency response rather than the compression. Because Group A and Group B consisted of different individuals who were randomly assigned to each group, it was not expected that the fine-tunings would be equal for the two groups, and in fact they were not. For the first fine-tuning, the average changes were 1 to 2 dB for Group B while the changes made for Group A at this session averaged less than 1 dB compared to the initial settings. Although the scope of this study does not allow for any conclusions on this point, it is conceivable that when the fine-tuning takes place face-to-face, the HCP might be better able to discern whether an issue is better addressed with a frequency response change or with counselling. In contrast, when the fine-tuning request is made remotely, the HCP has only the transmitted information to evaluate and act upon. There might be a greater tendency to respond with a change to hearing aid settings in this case, as observed in the slightly smaller changes for Group A at the first fine-tuning. At the second fine-tuning, the method was switched. Group A used ReSound Assist whereas Group B received face-to-face fine-tuning. For both groups, the final frequency response was further from the initial fitting than the fine-tuned settings at session 2. The overall magnitude of the average changes was 1 to 3 dB from the initial fitting. Overall, this suggests that HCPs may follow their usual strategies for fine-tuning such that one method does not result in significantly larger changes relative to the other method.
Usability of ReSound Assist
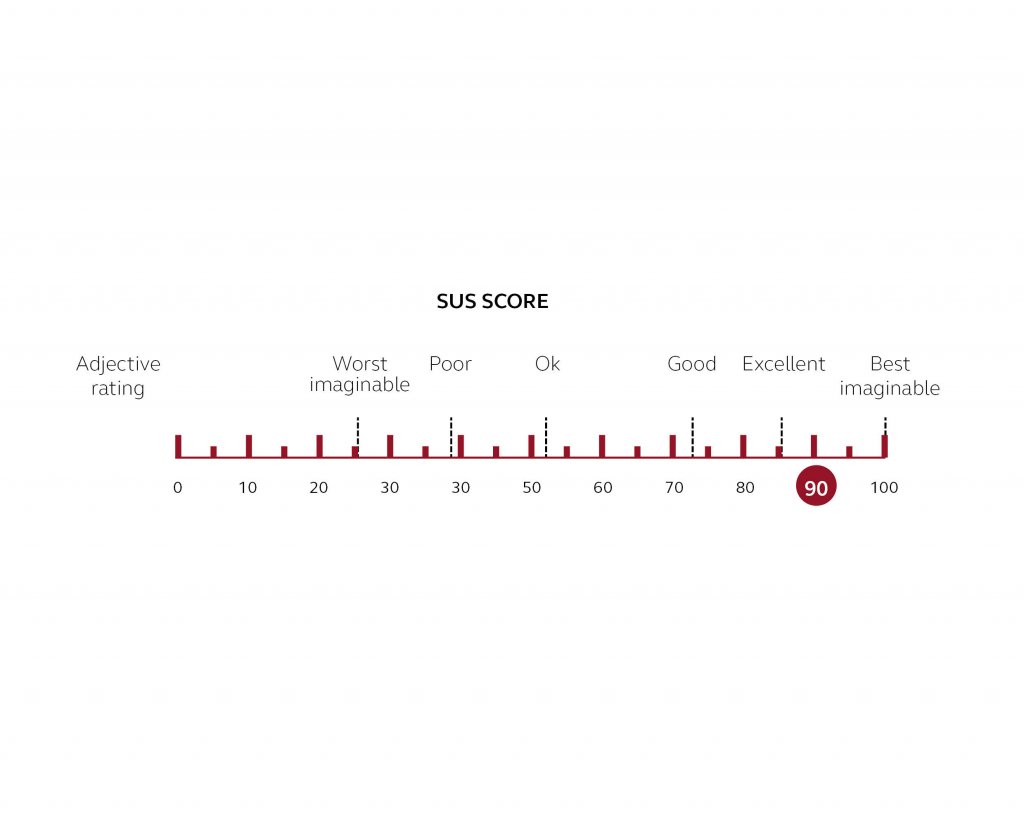
The median rating on the SUS was 90, indicating excellent usability of ReSound Assist. The 10 participants who owned compatible smartphones and continued the trial for the additional 4 weeks completed the SUS a final time at the conclusion of the trial, where the median rating was also 90. These findings are in agreement with an in-app survey of users conducted by ReSound, as well as a study with teenaged users15, where there was high agreement on the ease-of-use of ReSound Assist. As mentioned previously, it should be kept in mind that there is some selection bias in that participants in this trial as well as respondents in the other surveys were already smartphone users. Thus they can be assumed to show technology commitment that may be higher than the general population. This was in fact indicated by the technology commitment results in the current study. In actual clinical practice, more training and support may be required for new users to be able to competently use the technology if they are new to smartphones as well as hearing aids with teleaudiology features.
Comparison of fine-tuning in person and remotely
Apart from assessing outcomes with traditional measures, the two fine tuning methods were also evaluated qualitatively.
HCP-User dialogue face-to-face compared to remote
The face-to-face fine-tuning sessions were video recorded. The utterances of the HCP and participant for each session were transcribed and analyzed according to a version of the Roter Interaction Analysis System (RIAS) for coding medical dialogues that is adapted for analysis of dialogue structures in audiology.16 We substituted the original RIAS category “Facilitation and patient activation” with the category “Active Listening”. In most of the cases the audiologist was using utterances that fit to the concept where the listener reflects what has been said to confirm and deepen understanding. The sums and percentages of utterances by both the HCP and the participant are shown in Figure 6. Most of the HCP utterances were focused on “Data gathering” and “Active Listening”, while the majority of the participants’ utterances were in the “Information giving” category.
![]()
The two categories “data gathering” and “active listening” make up 70% of the utterances of the HCP. These two differ in motive and effect. While “data gathering” captures questions that explicitly deal with biomedical and psychosocial topics, the category “active listening” captures responses that prompt the participant to go into more detail with “Information giving”. It was observed that the identification of a problem usually started with a question categorized as “data gathering”, with follow-up responses and questions from the category “active listening”. From this realization, a meta-structure was deduced which could be compared with the meta structure of the interactions with the ReSound Assist feature. In face-to-face interactions, the HCP identifies and works through one issue at a time using first data-gathering and then active listening to elicit information giving from the user. This process repeats itself throughout the interaction as the HCP and user work through issues. In the ReSound Assist feature, data-gathering (by the feature) and information giving (by the user) is worked through in list-like fashion. At the end of this process, the feature emulates an active listening process by reflecting back to the user a summary of the data gathered. The user can at this point confirm and use free text to clarify information. The output of both types of interactions informs the clinical decisions and actions in the fine-tuning process.
Relative advantages and disadvantages of fine-tuning methods
Advantages of face-to-face interactions identified by the participants were the individual focus on their issues, the ability to precisely describe issues and the way in which an understanding of an issue can evolve organically through conversation. The personal interaction with the HCP was also valued as an advantage. For ReSound Assist, participants stressed convenience in terms of not needing to travel or make time for appointments. The ease-of-use in making requests and loading new settings into the hearing aids were also mentioned as advantages, although these aspects could be considered more as facilitators in making use of the technology. Disadvantages of both methods were the opposites of the advantages. For face-to-face interaction, there is the inconvenience of having to schedule and travel to appointments, as well as the time spent waiting for the HCP at the appointment. However, it was also mentioned that it can be difficult to recall and adequately describe issues that occur between appointments. Disadvantages that were named for ReSound Assist included the impersonal nature of the interaction, uncertainty with using the technology, and difficulty in describing the issue within the structured framework of the questionnaire in the feature.
Overall preference
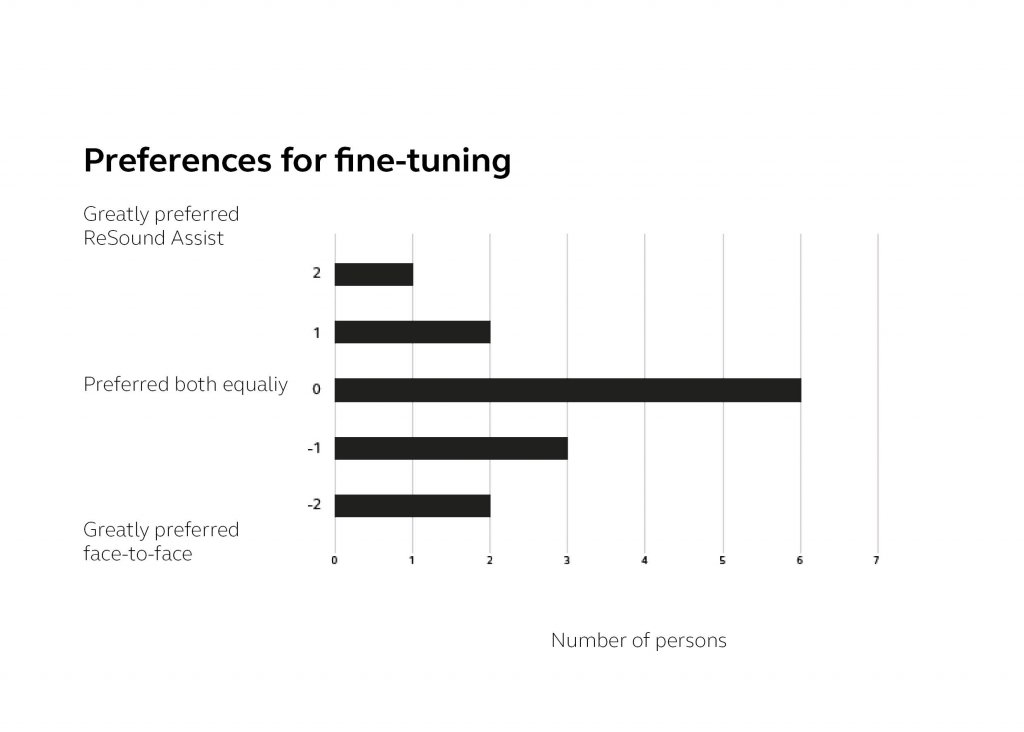
Participants indicated which fine-tuning method they preferred on a scale including strength of preference (Figure 7). No participants strongly favored either method. Most indicated no preference, while five participants had a weak-to-moderate preference for the face-to-face interaction and three had a weak-to-moderate preference for using ReSound Assist. This supports the use of ReSound Assist as a supplementary tool in hearing aid fitting that can increase access and convenience.
Summary
Teleaudiology has potential benefits for businesses, HCPs and hearing aid users, who are expected to increasingly demand such services. ReSound Assist is an asynchronous teleaudiology tool for fine-tuning that offers low barriers to implementation. However, it is important that such a teleaudiology service provide a comparable quality to the service performed in person. This study examined the question of quality by comparing the outcomes of fine-tunings done via ReSound Assist with in-person fine-tuning. It was found that speech-in-noise scores, fine-tuned changes, and subjective benefit with standardized questionnaires did not differ significantly for the two methods. Introducing the teleaudiology tool for use after the initial fitting and in-person follow up would fit in well with common clinical practice and might lead to the best outcomes considering that many potential users will have lower technology competence than the current group. Usability and user perception were also evaluated in the current trial. ReSound Assist was rated to be highly usable, and participants could easily identify advantages. Most indicated no preference for either ReSound Assist or face-to-face fine-tuning, supporting that the two methods can supplement each other as valuable components of hearing care.
References
- Montano J, Angley G, Ryan-Bane C, et al. eAudiology: Shifting from theory to practice. Hearing Review. 2018;25(9):20-24.
- Groth J, Bhatt M, Elsig Ravn P, Jahn A. Where does the day go? Insights from appointments in a large hearing aid practice. The Hearing Journal. June 7, 2017. Retrieved September 24, 2018 from https://journals.lww.com/thehearingjournal/blog/OnlineFirst/pages/post.aspx?PostID=13.
- Stender T, Fabry D. Teleaudiology: Friend or Foe in the Consumerism of Hearing Healthcare? Hearing Review. Published on May 10, 2017. Retrieved October 2, 2018 from http://www.hearingreview.com/2017/05/teleaudiology-friend-foe-consumerism-hearing-healthcare-2/.
- American Speech Language Hearing Association. Telepractice. Retrieved Sept 24, 2018 from https://www.asha.org/Practice-Portal/Professional-Issues/Telepractice/.
- Neyer FJ, Felber J, Gebhardt C. Entwicklung und validierung einer kurzskala zur erfassung von technikbereitschaft. Diagnostica. 2012; 58 (Mar): 87-99.
- Künemund H, Nele MT (2014): The technology acceptance puzzle – Findings from a Lower Saxony survey. Zeitschrift für Gerontologie und Geriatrie, 2014;47: 641-647 [doi 10.1007/s00391-014-0830-7M].
- Kollmeier B, Wesselkamp, M. Development and evaluation of a German sentence test for objective and subjective speech intelligibility assessment. J Acoust Soc Am. 1997;102(4): 2412-2421.
- Cox RM, Stephens D, Kramer SE. Translations of the international outcome inventory for hearing aids (IOI-HA): Traducciones del inventario internacional de resultados para auxiliares auditivos (IOI-HA). International Journal of Audiology. 2002 Jan 1;41(1):3-26.
- Noble W, Jensen NS, Naylor G, Bhullar N, Akeroyd MA. A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: The SSQ12. International Journal of Audiology. 2013 Jun 1;52(6):409-12.
- Schulte M, Vormann M, Meis M, Wagener K, Kollmeier B. Vergleich der Höranstrengung im Alltag und im Labor, 16. Jahrestagung der Deutschen Gesellschaft für Audiologie. 2013; CD-Rom, 5 pages, Rostock ISBN 978-3-9813141-3-7.
- Schulte, M., Habicht, J., Neher, T., Meis, M., and Wagener, KC. “Entwicklung der Höranstrengung im Alltag nach Erstversorgung mit Hörgeräten,” Jahrestagung der Dt. Ges. für Audiologie (DGA). 2016: 91.
- Bangor A, Kortum P, Miller J. Determining What Individual SUS Scores Mean: Adding an Adjective Rating Scale. Journal of Usability Studies. 2009; 4(3): 114-123.
- Humes LE, Wilson DL, Barlow NN, Garner CB, Amos N. Longitudinal changes in hearing aid satisfaction and usage in the elderly over a period of one or two years after hearing aid delivery. Ear & Hearing. 2002 Oct 1;23(5):428-38.
- Bentler RA, Niebuhr DP, Getta JP, Anderson CV. Longitudinal study of hearing aid effectiveness. II: Subjective measures. Journal of Speech, Language, and Hearing Research. 1993;36(4):820-31.
- Quilter M, Pick K, Haastrup A. Examining potential applications for pediatric telehealth and remote fine-tuning. Paper presented at Hearing Across the Lifespan, 2018 June 7-9; Cernobbio, Lake Como, Italy.
- Grenness C, Hickson L, Laplante-Lévesque A, Meyer C, Davidson B. The nature of communication throughout diagnosis and management planning in initial audiologic rehabilitation consultations. Journal of the American Academy of Audiology; 26(1):36-50.