Canadian Vestibular Audiologists: Connecting Through Cases & Discussion

Editor’s Note:
In this edition of “Striking the Right Balance,” Carolyn Falls & Curtis Wetmore, MSc, Aud(C), Reg CASLPO introduce an interesting vestibular case that will be discussed in further detail during an upcoming Facebook Live event (hosted by the CAA National Vestibular Special Interest Group).
Michael Vekasi, AuD, R.Aud, Aud(C), FAAA and Erica Zaia, MSc, RAUD are coordinating the “Striking the Right Balance,” feature which will cover the latest information on ‘all things vestibular.’
If you would like to be more involved in all things vestibular, please check out and like our Facebook page by searching for “CAA National Vestibular Special Interest Group” within Facebook. You can also reach us by email at CAAvestibular@gmail.com.
Working as a vestibular audiologist can be a strange and lonely pursuit. There aren’t that many of us, we have a lot to learn, and there’s a high probability of getting blank stares from anyone you try to talk to about it. So what is an audiologist to do when there’s no one around to discuss interesting cases?
The CAA National Vestibular Special Interest Group has you covered. On November 30th at 7:00 PM ET, we will be hosting a live case presentation and discussion for all Canadian audiologists interested in vestibular practice, presented by the team at Toronto General Hospital. Mark your calendars.
We hope that this will be the first in a regular series of virtual meetings to build knowledge and a strong community of vestibular audiologists across Canada. So stop whatever you’re doing RIGHT NOW and join our Facebook group to ensure you don’t miss anything.
Beyond announcements for virtual meetings, the group will also serve as a virtual forum for posting and discussing interesting vestibular findings.
Sneak Peek
We think the chance to discuss an interesting case with other vestibular audiologists is something you won’t want to miss, but don’t take our word for it: here’s a sneak peek into the first case we will discuss.
Background
A 40-year-old man was referred by the ER to the Hearing & Balance Centre at Toronto General Hospital for a hearing test. The patient did not have any hearing complaints or tinnitus. His primary complaint was vertigo, which was the reason for his visit to the ER about 4 days earlier. The patient reported significant issues with dizziness and imbalance and was also visibly off-balance in the clinic. An urgent consultation with ENT was arranged, which resulted in a diagnosis of Vestibular Neuritis. The patient presented back to the clinic two weeks later for a comprehensive vestibular evaluation. The hearing assessment was normal.
Test Results
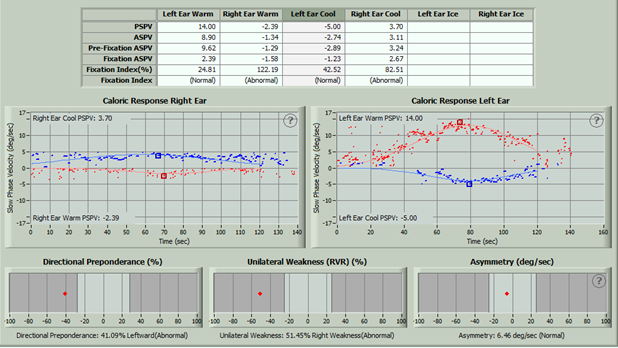
Videonystagmography (VNG): Normal oculomotor testing with absent positional nystagmus and negative Dix-Hallpike. However, positive post-head shake nystagmus (~6 deg/sec LBN) and caloric testing revealed a 51% right weakness.
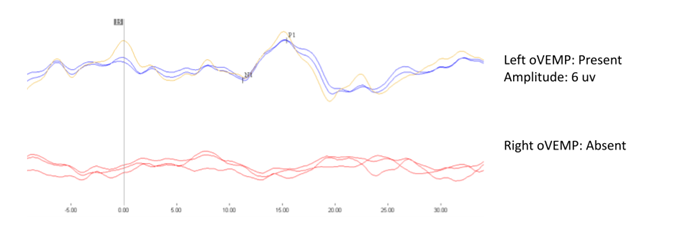
Vestibular Evoked Myogenic Potentials (VEMP): cVEMP results were normal and symmetrical bilaterally. oVEMPs were normal on the left but absent on the right (see figure 2).
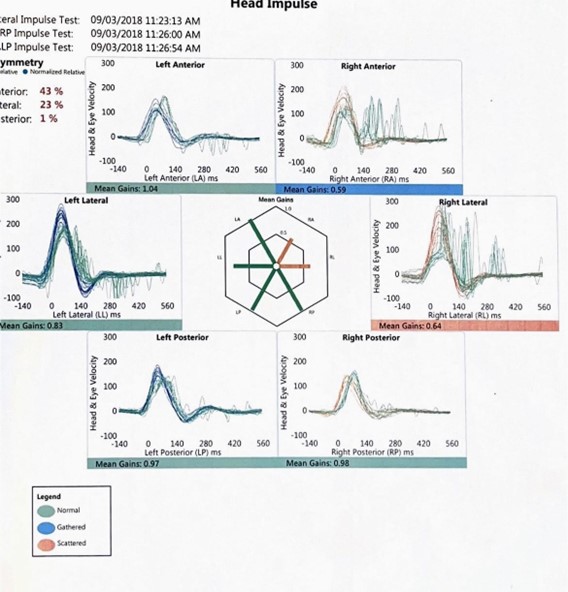
Video Head Impulse Test (vHIT): Results indicated a VOR loss for the right lateral and anterior canals. The results were normal for the right posterior canal and all canals on the left.
Analysis
The original diagnosis from the ENT consultation was right Vestibular Neuritis. However, we could localize the neuritis to the superior branch of the right vestibular nerve through laboratory vestibular testing. The vestibular nerve has a superior branch, which innervates the anterior and horizontal canals and the utricle, and an inferior branch which innervates the posterior canal and the saccule. Therefore, the normal findings for the right cVEMP and posterior semicircular canal, combined with the abnormal findings for the right oVEMP and right anterior/lateral semicircular canals were consistent with neuritis of the superior branch of the vestibular nerve.
Don’t forget to join the Facebook Group. See you on November 30th at 7 PM ET.