The Digit Triplet Test: A Canadian Version

Help-seeking for hearing loss in adults is a long process. For example, it can take 10 years for adults to seek help after the first signs of hearing loss are noticed.1,2 This delay in seeking help has been attributed to different factors, including the negative association of hearing loss with ageing3 or cognitive impairment,4,5 as well as limited access to service6and unperceived hearing loss.7 In a recent national survey, 77% of Canadian adults between the ages of 40 and 79 years who were found to have a uni- or bilateral pure-tone average threshold greater than 25 dB HL in the high frequencies (3, 4, 6 and 8 kHz) were not aware of their hearing loss.7 Although there are a number of reasons for waiting so long before seeking help,3–10 this high prevalence of unperceived hearing loss suggests the importance of increasing awareness. Furthermore, unacknowledged or unaddressed hearing loss can increase risk for cognitive decline and social isolation.11 Regular screening has been suggested as one strategy to bring individuals with hearing loss to consult earlier than they presently do, and to prevent the negative effects of hearing loss on their quality of life.7,12,13
The Digit Triplet Test (DTT)14 was originally developed in Dutch for the purpose of hearing screening and to promote help-seeking. The DTT is a speech-in-noise screening test that uses combinations of three digits as speech material, also called digit triplets. The test uses an adaptive procedure to determine the speech reception threshold (SRT). The SRT corresponds to the speech-to-noise ratio at which 50% of the triplets are correctly recognized. The DTT was initially developed for self-assessment via telephone, but it is now available over a wide range of platforms including smartphones and personal computers. It has been adapted in about 15 different languages or dialects.15
A Canadian Version
A Canadian version16 of the Digit Triplets Test (CDTT) was been developed by a team of researchers at the University of Ottawa and Toronto. The test is available in both official languages, English and French, and testing can be conducted using a female or male talker. Following ICRA recommendations,17 only digits with the same number of syllables were retained: digits “zero” and “seven” were excluded in English, and “zéro” and “quatre” in French. Each version of the CDTT (English-Male, English-Female, French-Male, and French-Female) includes four lists of 24 triplets. The lists are counterbalanced so that each digit occurs three times in each triplet position, without repetition of the same digit within a triplet. The presentation order of the 24 triplets is randomized on each run of a list. Testing is carried out in speech-shaped noise matching the long-term average spectrum of the digit material for each language-talker version of the CDTT. Test administration is about 2–3 minutes when using the binaural condition and adaptive procedure.
The CDTT software was developed as a cross-platform Java desktop application and it can be run on any major operating system (e.g., Windows, Mac OS, Linux). The main interface provides controls for the test operator to enter participant information, select test parameters, run a test, and save the results (Figure 1). The participant can enter their responses on an external USB numeric keypad, or on a keypad that is displayed on the screen as the test is running. A USB sound card is used for portability and reproducibility across computers and sound playback hardware. The use of Radioear DD45 earphones is recommended as normative data were obtained with this grade of earphones. Results obtained to date suggest that hearing screening can be conducted with these earphones in areas with background noise levels not exceeding 60 dBA, while the use of circumaural earphones might be considered in areas with noise levels up to 80 dBA.
Figure 1. Canadian Digit Triplet Test interface (top), the response keypad (bottom left) and hardware set up (bottom right).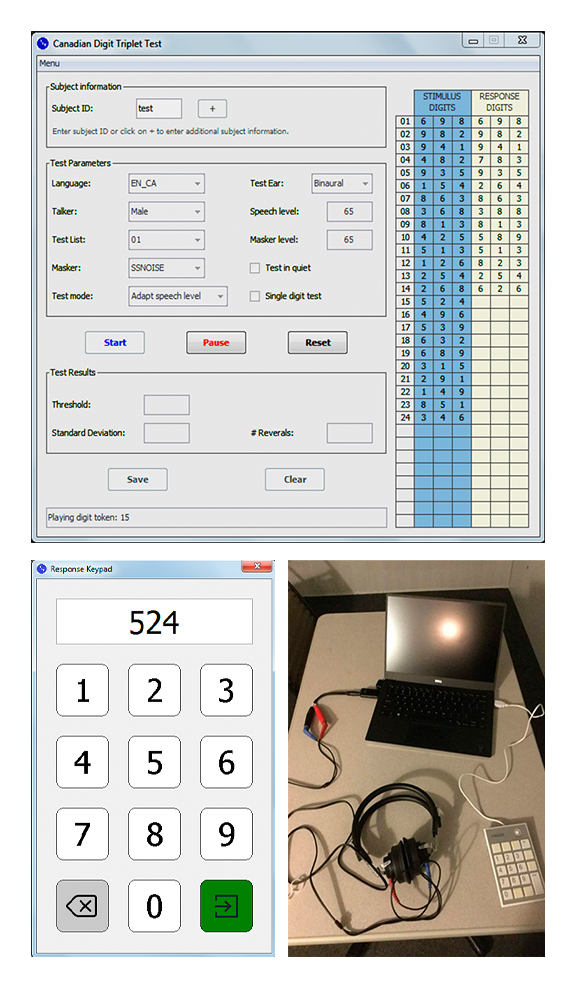
Effect of Age
Child Populations
A cohort of Francophone children between the ages of 5 and 12 with normal hearing thresholds were recruited at the École Régionale Saint-Basile (St-Basile, NB) to determine the effect of child development on the CDTT test results. Participants of this cohort were tested with both the French-Female and French-Male versions of the test, in a quiet room at the school. The mean SRT obtained with the 8-9 year-old group (n= 22) and the 11–12 year-old group (n=23) was similar for the two versions, ranging from −10.5 to −11.2 dB SNR. Not surprisingly, the test-retest standard deviation (1.2 dB) was about twice the value of the adult participants (see above). The results revealed that the actual test paradigm was too difficult for the youngest group (5–6 years).
A similar study was conducted at the Eenchokay Birchstick School (Pikangikum First Nations, ON) with 84 children from 8 to 9 years of age. Pikangikum has a 97% retention rate of Ojibway language. As such, Ojibway is the first language learned by most children, and English is learned during their first years of schooling. Participants of this cohort were tested with the English female voice (n=39) or English male voice (n=39, different children) of the CDTT in a quiet room at the school. The mean SRT was similar for both versions, ranging from −8.8 to −9.4 dB SNR. The test-retest standard deviation was in the order of 2 dB for this specific group of children, which is about thrice the adult’s value. Further testing is required before arriving to any conclusion, but the participants’ linguistic background may explain the higher variability of results within this cohort of children.
Older Adults
A cohort of 16 older adults (range 63-82 years old) with hearing thresholds in the normal range (mean PTA = 10 dB HL) were tested to determine the effect of aging on CDTT test results using the English Male version of the CDTT. The results of the older adults were compared to the normative test group of young normal hearing listeners (mean PTA = 1 dB HL). There was a small but significant difference between the two groups, with older listeners having a mean SRT that was 0.5 dB higher than the mean SRT of younger listeners. The test-retest standard deviation and the other properties of the test were the same in both age groups. Results indicate that the test can reliably be administered with older adults, but correction factors due to age or residual differences in hearing thresholds may be required.
The CDTT is presently being used in two large-scale multi-site studies on aging across Canada: the Canadian Consortium on Neurodegeneration in Aging (CCNA: http://ccna-ccnv.ca/en/) and the Canadian Longitudinal Study on Aging (CLSA: https://www.clsa-elcv.ca/). In addition to audiometry, the CDTT is being used in CCNA and CLSA to investigate sensory-cognitive links in aging. The CDTT is also being used by several other Canadian research groups who are investigating links between hearing loss and age-related declines in other domains such as vision and balance.
Conclusion
Hearing loss in adults has been associated with social isolation,18 depression,19 cognitive decline,20 and dementia. Early identification is important for prevention and early intervention. However, help seeking for hearing loss is a long process, and often delayed. 3–9Unperceived hearing loss has been identified as one of the reasons of the delay in help seeking, especially among Canadians between the ages of 40 to 79 years with hearing loss in the high-frequency range.7 Routine hearing screening in primary care has been suggested as one strategy to increase awareness of unperceived hearing loss.7,13 Automatic hearing screening tools, such as the CDTT, could ultimately be adopted to promote healthy aging and contribute to averting the consequences of hearing loss.
Compared to pure-tone screening, which has traditionally been used for detection of hearing impairment, the CDTT can be used in less favorable acoustic conditions and is automatic. The CDTT includes a female and a male talker for both the French and the English version of the test, which provides a unique set of speech test stimuli for use in Canada. Its versatile testing platform offers the possibility to conduct the test in different environments (e.g., waiting rooms, pharmacies) and conditions (e.g., monaural or binaural, adaptive or fixed levels procedures). Additional validation steps are needed to establish age-specific norms for children and older adults, as well as non-native speaker of French or English and those with comorbid conditions such as vision, motor, and memory loss. Ongoing research will provide evidence to guide new approaches to health promotion and clinical practice in primary care and specialized settings such as schools and long-term care facilities.
Acknowledgments
This work was supported in part by grants from the Natural Sciences and Engineering Research Council (NSERC) to C.G. and M.K.P.-F. The authors thank the two talkers who participated in the recording of the digit stimuli. Students at the University of Toronto (Mississauga) and University of Ottawa are gratefully acknowledged for their assistance in data collection.
Portions of this article were presented at the SAC Audiology Event in May 2019 (Montreal, QC) and at the at the 26th International Congress on Sound and Vibration in Montréal (QC) in July 2019.
References
- Davis A. Hearing in adults: the prevalence and distribution of hearing impairment and reported hearing disability in the MRC Institute of Hearing Research's National Study of Hearing: Whurr Publishers London; 1995.
- Kochkin S. MarkeTrak VIII: 25-year trends in the hearing health market. Hear Rev 2009;16(11):12–31.
- Wallhagen MI. The stigma of hearing loss. The Gerontologist. 2010;50(1):66-75.
- Gagné J-P, Jennings MB, Southall K. Understanding the stigma associated with hearing loss in older adults. Hearing Care Adults 2009:203–12.
- Kochkin S. MarkeTrak VII: Obstacles to adult non-user adoption of hearing aids. Hear J 2007;60(4):24–51.
- McColl MA, Jarzynowska A, Shortt S. Unmet health care needs of people with disabilities: population level evidence. Disabil Soc 2010;25(2):205–18.
- Ramage-Morin PL, Banks R, Pineault D, Atrach M. Unperceived hearing loss among Canadians aged 40 to 79. Health Rep 2019;30(08):11–20.
- Hetu R, Riverin L, Getty L, Lalande N, St-Cyr C. The reluctance to acknowledge hearing difficulties among hearing-impaired workers. Br J Audiol 1990;24(4):265–76.
- Laplante-Lévesque A, Brännström KJ, Ingo E, Andersson G, Lunner T. Stages of change in adults who have failed an online hearing screening. Ear Hear 2015;36(1):92–101.
- Vestergaard Knudsen L, Öberg M, Nielsen C, Naylor G, Kramer SE. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: A review of the literature. Trends Amplificat 2010;14(3):127-54.
- Mick P, Pichora-Fuller MK. Is hearing loss associated with poorer health in older adults who might benefit from hearing screening? Ear Hear 2016;37(3):e194-e201.
- Ratanjee-Vanmali H, Swanepoel DW, Laplante-Lévesque A. Characteristics, behaviours and readiness of persons seeking hearing healthcare online. Internat J Audiol 2019;58(2):107-15.
- Davis A, McMahon CM, Pichora-Fuller KM, Russ S, Lin F, Olusanya BO, et al. Aging and hearing health: the life-course approach. Gerontologist 2016;56(Suppl_2):S256–S67.
- Smits C, Kapteyn TS, Houtgast T. Development and validation of an automatic speech-in-noise screening test by telephone. Int J Audiol. 2004;43(1):15-28.
- Denys S, Hofmann M, Luts H, Guerin C, Keymeulen A, Van Hoeck K, et al. School-Age Hearing Screening Based on Speech-in-Noise Perception Using the Digit Triplet Test. Ear Hear. 2018;39(6):1104-15.
- Giguère C, Lagacé J, Ellaham NN, Pichora-Fuller MK, Goy H, Bégin C, et al. Development of the Canadian Digit Triplet Test in English and French. J Acoust Soc Am 2020;147(3):EL252–EL8.
- Akeroyd MA, Arlinger S, Bentler RA, Boothroyd A, Dillier N, Dreschler WA, et al. International Collegium of Rehabilitative Audiology (ICRA) recommendations for the construction of multilingual speech tests. ICRA Working Group on Multilingual Speech Tests. Int J Audiol. 2015;54 Suppl 2:17-22.
- Stam M, Smit JH, Twisk JW, Lemke U, Smits C, Festen JM, et al. Change in psychosocial health status over 5 years in relation to adults’ hearing ability in noise. Ear Hear 2016;37(6):680–9.
- Huang C-Q, Dong B-R, Lu Z-C, Yue J-R, Liu Q-X. Chronic diseases and risk for depression in old age: A meta-analysis of published literature. Ageing Res Rev 2010;9(2):131–41.
- Gosselin PA, Ismail Z, Faris PD, Benkoczi CL, Fraser TL, Cherry SW, et al. Effect of hearing ability and mild behavioural impairment on MoCA and memory index scores. Can Geriatr J 2019;22(3):165.