A Narrative Review of Air-Conduction Re-routing Systems for Adults with Limited Useable Hearing Unilaterally

Disclosures: Portions of this work was sponsored by Phonak, AG
Introduction
Clinical management of adults who have unilateral hearing loss can be difficult. There are listening situations where they may be able to communicate easily and others where listening is very difficult [1]. The difference between these situations is related to many factors, including the location of the talker relative to the ear with hearing loss, the presence and location of background noise, the degree of reverberation, and so on. This can lead to frustration, avoiding social situations, and mental fatigue [2]. These challenges might be even more significant for adults with limited useable hearing unilaterally (also known as single-sided deafness). Yet, finding the optimal clinical intervention is difficult.
Many adults with limited useable hearing unilaterally (LUHU) do not pursue amplification [3, 4], perhaps because their unilateral hearing is sufficient in many typical listening situations (e.g., in a quiet office or at home watching television). For those who do seek an intervention, technological options are limited to re-routing systems (either wireless air conduction or bone conduction) and, more recently, unilateral cochlear implants. Re-routing systems work by placing a transmitter on the ear with LUHU, which re-routes the sound from that side of the head to the other cochlea. Air-conduction re-routing systems, hereafter referred to as contralateral routing of signals (CROS) systems, rely on two acoustic devices: a transmitter on the ear with LUHU and a receiver on the ear with better hearing. Bone conduction devices (BCDs) work with a bone conduction device on the side of the head with LUHU and re-route the signal via bone conduction to the cochlea with better hearing. A fourth option, bilateral CROS or a BiCROS, is available for adults with hearing loss in the ear with better hearing and who could benefit from traditional amplification and re-routing.
These re-routing systems have been around for decades. However, their form and function have advanced considerably since the initial devices were introduced (see Taylor [5] for a review of re-routing options and their history). Despite their long availability history, CROS/BiCROS systems are not commonly fit devices [6]. Even busy clinics might only see a few patients a year who have LUHU [7]. Therefore, many clinicians might not be familiar with the evidence supporting CROS/BiCROS fittings. The purpose of this paper was to conduct a narrative review of the evidence supporting air-conduction re-routing systems for adults with LUHU, specifically CROS and BiCROS systems.
Materials and Methods
The National Institutes of Health PubMed database was searched and articles were included if they were published before August 20, 2023. The search keywords included ‘CROS,’ ‘contralateral routing of signals,’ or ‘BiCROS.’ The title and abstract of the articles were screened. Additional articles were identified via forward and backward search of the reference lists of the identified articles. Articles were included for final review based on the PICO framework. Specifically, the study population needed to include adults with LUHU (with or without hearing loss in the contralateral ear); the study intervention needed to be an air-conduction, re-routing system (CROS or BiCROS); the study comparison had to be a standard condition (either no device or traditional device such as a unilateral hearing aid); the study outcomes needed to include either behavioral testing in the laboratory (speech recognition or localization), communication questionnaire results (e.g., subjective ratings of listening abilities at home), device acceptance, or device use.
Results
Initially, 108 articles were retrieved. Review of the titles and abstracts excluded 75 articles. Specifically, articles were excluded if they focused only on implantable solutions (n = 37), included only pediatric participants (n = 13), did not include participants with hearing loss (n = 13), were review articles (n = 7), were not in English (n = 4), were published protocols (n = 2) or did not include behavioural or subjective listening as outcomes (n = 1). As a result, 32 publications met the inclusion criteria. From those 32, forward and backward search of their reference lists revealed an additional 5 studies for inclusion. Therefore, the total number of included studies in the review was 37. For this review, studies were classified based on the research questions they addressed: CROS/BiCROS benefits in general, CROS/BiCROS compared to surgical implants, and clinical decisions that could affect CROS/BiCROS benefits. Figure 1 displays the proportion of studies whose research questions fall into each category.
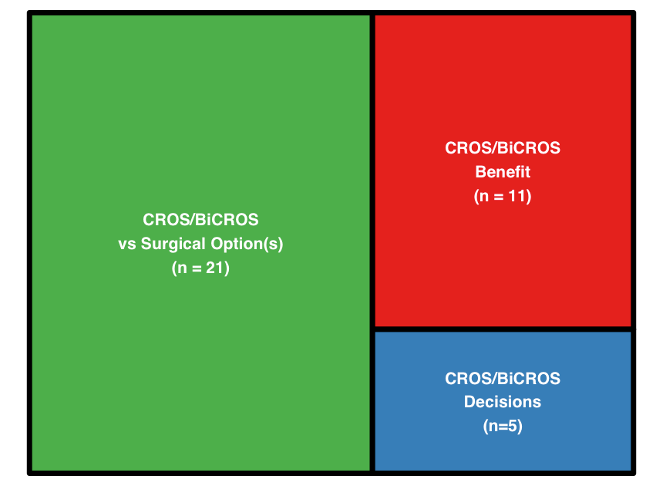
CROS/BiCROS Benefit
Eleven studies explicitly evaluated CROS/BiCROS benefits or use time. The results of 5 studies generally suggest that CROS/BiCROS systems can improve speech recognition when speech is directed toward the ear with LUHU but can impair performance when speech is directed toward the ear with better hearing, especially in noise [8-12]. One study demonstrated BiCROS benefits relative to a monaural hearing aid for adults with LUHU and aidable hearing in the contralateral ear [13].
In addition, 5 studies investigated subjective perception of CROS/BiCROS use in daily life and/or use time; these studies suggest that use times are generally high for people who choose to use their device [9, 14-16]. A relatively high percentage (60–80%) of participants chose to use their re-routing devices [9, 15, 17], although device acceptance rates for BiCROS have been reported to be lower than CROS acceptance rates [e.g., 26%; 18]. Combined, these results support benefits of CROS/BiCROS systems noted only in specific laboratory environments and generally high CROS use by participants outside the laboratory. However, one theme from the literature was variable device use and acceptance across participants.
CROS/BiCROS Compared to Surgical Implants
Fifteen studies investigated the difference between CROS/BiCROS and BCDs for adults with LUHU. These studies revealed the expected effects of CROS/BiCROS systems, which are beneficial when the speech is presented to the ear with LUHU, but can impair performance when the speech is presented toward the ear with better hearing [19-33]. In addition to unaided comparisons, they compared performance with CROS/BiCROS to BCDs, where the results were mixed. Some studies have suggested people perform better with CROS/BiCROS than with BCDs [28-30], whereas some have found relatively equivalent results between devices [23-27]. However, most studies demonstrate that performance or subjective experiences are better with BCDs than with CROS/BiCROS devices [19-22, 31-34]. Differences between studies that demonstrate CROS/BiCROS versus BCD benefits might be related to the technology under study or participant selection bias [35, 36].
Seven studies compared outcomes and performance between CROS/BiCROS and cochlear implants. Results of these studies suggest that, unlike CROS/BiCROS or BCDs, cochlear implants can provide bilateral hearing for participants with LUHU [30, 31, 37-39]. However, in two studies where participants chose their intervention, CROS was chosen more often than cochlear implants [40, 41].
Clinical Decisions
Only 5 studies addressed changes an audiologist could make to the CROS/BiCROS system to maximize benefits, although not all of them might be relevant with modern devices. For example, Courtois and Jensen [42] manipulated the tube diameter, which affects the receiver frequency response. Ultimately, Courtois & Jensen recommend that dispensers trial different tube lengths (and thus frequency characteristics and venting effects) to balance unaided hearing and the introduction of noise. With modern instruments, different gain characteristics can be manipulated digitally, although venting continues to be a factor worthy of serious consideration.
More recently, Williams, McArdle [43] studied the effect of fitting a new, modern BiCROS (with advanced directionality) compared to BiCROS users’ own systems (which had less advanced technology). The authors reported that the newer, more modern BiCROS system improved performance and subjective ratings compared to the older BiCROS systems. Similarly, Valente and Oeding [44] said advanced directionality for BiCROS systems can improve speech recognition performance in some conditions, especially in diffuse noise. However, the authors also noted that directional microphones could impair speech recognition performance if the directional microphone was on the transmitter and the speech was near the transmitter. This finding suggests that directionality decisions must be made carefully and likely adaptive to the listening environment.
Digital noise reduction can also be effective in CROS systems. Although Oeding and Valente [45] reported that digital noise reduction in a BiCROS system did improve speech recognition performance, they reported it did improve subjective ratings. Finally, Kuk, Seper [46] reported that providing an on/off switch for the transmitter, combined with counseling about the switch, improved speech recognition performance and subjective ratings. When combined, these studies suggest there are steps that audiologists and manufacturers can take to optimize benefits of CROS/BiCROS systems for adults with LUHU.
Discussion
The purpose of this narrative review was to summarize the evidence supporting non-surgical, air-conduction re-routing systems for adults with LUHU. The results demonstrate that there are many peer-reviewed papers addressing CROS/BiCROS. Still, most research efforts have been devoted to comparing CROS/BiCROS to surgical solutions (bone conduction or cochlear implants) or unaided conditions (see Figure 1). Far fewer research articles address research questions related to actions audiologists could take in fitting these systems. The available peer-reviewed evidence on this topic suggests that:
- There is variability in CROS/BiCROS acceptance and use, so audiologists could ensure patients have adequate trial periods with such systems.
- Modern systems are likely more beneficial than older systems, so audiologists could strive to fit modern systems.
- Noise reduction in CROS/BiCROS can improve subjective outcomes, so audiologists could ensure noise reduction is active.
- The fitting of advanced directionality can be beneficial, so audiologists could activate microphone directionality, but considerations for specific listening situations should be considered (e.g., ensuring the microphone is adaptive).
- An accessible on/off switch on the transmitter and appropriate counseling can increase CROS/BiCROS benefit, so audiologists could consider providing this manually accessible switch and training on its use.
Clearly these learnings from the literature are not comprehensive enough to make fully evidence-based clinical decisions. The literature is more than 8 years old, and reflects only a few participants with a few outcomes. However, the results of this narrative review are consistent with recent guidelines on managing severe-to-profound hearing loss in adults [47], where the authors’ recommendations for managing LUHU are based on 9 articles, only 6 of which were peer-reviewed scientific papers. Thus, the field would benefit from additional rigorous scientific evaluation to support clinical decisions with CROS/BiCROS. Specific areas include, but are not limited to, setting directional microphones and including representative listening situations.
Microphone Directionality
There is very limited work examining microphone setting in CROS/BiCROS systems, except where noted above. Conversely, there are a plethora of studies investigating advanced directionality for adults with bilateral hearing loss [48, 49], even in asymmetric fittings [50, 51] or asymmetric listening environments [e.g., 52, 53, 54]. However, directionality should be explicitly evaluated with CROS/BiCROS fittings because, as shown by Valente and Oeding [44], directionality can interfere with the function of a re-routing system if the directional microphone is attenuating sounds of interest directed at the ear with LUHU. An adaptive microphone and/or an automatic switching algorithm would be necessary to avoid placing important signals in microphone nulls. Alternatively, Kuk, Seper [46] have demonstrated that a manual switch and some training successfully avoided some of the pitfalls associated with CROS/BiCROS use. Perhaps this work could be extended to consider steerable directivity in re-routing systems or systems with reverse cardioid microphone patterns for specific situations where directionality and CROS/BiCROS use are incompatible [55].
Representative Listening Situations
Although there are recommendations for standardizing evaluation protocols across sites [56], it seems practical to expand the types of listening situations under investigation to include those more representative of listening situations that are typical and/or important to adults in their daily lives. Most adults do not listen to auditory-only speech toward one ear and noise directed toward the other ear. Real-life situations include multiple sources of rich information that can be helpful for communication but are rarely represented in research with CROS/BiCROS systems. Examples of such information could include visual cues [57, 58], head-turning [59, 60], and situational contextual cues [61]. Without such studies, it is unclear how the laboratory investigations translate into expected benefits in daily life.
Conclusions
The purpose of this paper was to review the evidence supporting CROS/BiCROS fittings for adults with limited useable hearing unilaterally (LUHU, also known as single-sided deafness). The review reveals that the literature has many studies investigating CROS/BiCROS benefits and comparing these benefits to surgical intervention options (BCDs and cochlear implants). However, the literature provides limited advice for audiologists fitting these systems. Additional work is warranted to further refine our understanding of directionality and the applicability of these findings to real-world listening environments enriched with cues that support communication (context, visual cues, head turning). In the meantime, the existing evidence supports an adequate trial period with CROS/BiCROS before committing to purchase, the use of digital noise reduction, advanced directionality (ideally adaptive directionality), and the use of a switch for deactivating the transmitter, when appropriate based on the listening environment.
References
- Katiri, R., et al., Device-based interventions that seek to restore bilateral and binaural hearing in adults with single-sided deafness: a conceptual analysis. Frontiers in Audiology and Otology, 2023. 1: p. 1242196.
- Alhanbali, S., et al., Self-reported listening-related effort and fatigue in hearing-impaired adults. Ear and Hearing, 2017. 38(1): p. e39-e48.
- Drusin, M.A., et al., Trends in hearing rehabilitation use among vestibular schwannoma patients. Laryngoscope, 2020. 130(6): p. 1558-1564.
- Macielak, R.J., et al., Hearing Status and Aural Rehabilitative Profile of 878 Patients With Sporadic Vestibular Schwannoma. Laryngoscope, 2021. 131(6): p. 1378-1381.
- Taylor, B., Contralateral routing of the signal amplification strategies. Seminars in Hearing, 2010. 31(04): p. 378-392.
- Hickson, L., S. Clutterbuck, and A. Khan, Factors associated with hearing aid fitting outcomes on the IOI-HA. International Journal of Audiology, 2010. 49(8): p. 586-595.
- Hayes, D., A Practical Guide to CROS/BiCROS Fittings. Audiology Online, 2006.
- Harford, E. and J. Barry, A rehabilitative approach to the problem of unilateral hearing impairment: The contralateral routing of signals (CROS). Journal of Speech and Hearing Disorders, 1965. 30: p. 121-38.
- Ericson, H., et al., Contralateral routing of signals in unilateral hearing impairment. A better method of fitting. Scand Audiol, 1988. 17(2): p. 111-6.
- Ryu, N.G., et al., Clinical effectiveness of wireless CROS (contralateral routing of offside signals) hearing aids. Eur Arch Otorhinolaryngol, 2015. 272(9): p. 2213-9.
- Lundborg, T., I. Swärd, and B. Lindström, Experience with Classic Cros Hearing Aids in Unilateral Deafness. Scandinavian Audiology, 1976. 5(1): p. 17-23.
- Lotterman, S.H. and R.N. Kasten, Examination of the CROS type hearing aid. Journal of Speech and Hearing Research, 1971. 14(2): p. 416-420.
- Del Dot, J., L.M. Hickson, and B. O’Connell, Speech perception in noise with BICROS hearing aids. Scand Audiol, 1992. 21(4): p. 261-4.
- Gelfand, S.A., Usage of CROS hearing aids by unilaterally deaf patients. Arch Otolaryngol, 1979. 105(6): p. 328-32.
- Aufricht, H., A Follow-Up Study of the CROS Hearing Aid. Journal of Speech and Hearing Disorders, 1972. 37(1): p. 113-117.
- Busk Linnebjerg, L. and R. Wetke, The benefits of CROS aids for individuals with unilateral sensorineural hearing loss. Hearing, balance and communication, 2014. 12(1): p. 36-40.
- Hill, S.L., 3rd, et al., Assessment of patient satisfaction with various configurations of digital CROS and BiCROS hearing aids. Ear Nose Throat J, 2006. 85(7): p. 427-30, 442.
- Seong, J., et al., Clinical Factors Influencing the Trial and Purchase of Bilateral Microphones with Contralateral Routing of Signal in Patients with Asymmetric Sensorineural Hearing Loss. J Audiol Otol, 2020. 24(1): p. 29-34.
- Niparko, J.K., K.M. Cox, and L.R. Lustig, Comparison of the bone anchored hearing aid implantable hearing device with contralateral routing of offside signal amplification in the rehabilitation of unilateral deafness. Otol Neurotol, 2003. 24(1): p. 73-8.
- Wazen, J.J., et al., Transcranial contralateral cochlear stimulation in unilateral deafness. Otolaryngol Head Neck Surg, 2003. 129(3): p. 248-54.
- Hol, M.K., et al., Bone-anchored hearing aid in unilateral inner ear deafness: a study of 20 patients. Audiol Neurootol, 2004. 9(5): p. 274-81.
- Lin, L.M., et al., Amplification in the rehabilitation of unilateral deafness: speech in noise and directional hearing effects with bone-anchored hearing and contralateral routing of signal amplification. Otol Neurotol, 2006. 27(2): p. 172-82.
- Finbow, J., et al., A Comparison Between Wireless CROS and Bone-anchored Hearing Devices for Single-sided Deafness: A Pilot Study. Otol Neurotol, 2015. 36(5): p. 819-25.
- Leterme, G., et al., Contralateral routing of signal hearing aid versus transcutaneous bone conduction in single-sided deafness. Audiol Neurootol, 2015. 20(4): p. 251-60.
- Snapp, H.A., et al., Effectiveness in Rehabilitation of Current Wireless CROS Technology in Experienced Bone-Anchored Implant Users. Otol Neurotol, 2017. 38(10): p. 1397-1404.
- Snapp, H.A., et al., Comparison of Speech-in-Noise and Localization Benefits in Unilateral Hearing Loss Subjects Using Contralateral Routing of Signal Hearing Aids or Bone-Anchored Implants. Otol Neurotol, 2017. 38(1): p. 11-18.
- Mertens, G., et al., A Prospective Randomized Crossover Study in Single Sided Deafness on the New Non-Invasive Adhesive Bone Conduction Hearing System. Otol Neurotol, 2018. 39(8): p. 940-949.
- Choi, J.E., et al., A comparison between wireless CROS/BiCROS and soft-band BAHA for patients with unilateral hearing loss. PLoS One, 2019. 14(2): p. e0212503.
- Fogels, J., et al., Single-Sided Deafness-Outcomes of Three Interventions for Profound Unilateral Sensorineural Hearing Loss: A Randomized Clinical Trial. Otol Neurotol, 2020. 41(6): p. 736-744.
- Kurz, A., et al., Evaluating the Decision for Cochlear Implantation in Individuals With Single-Sided Deafness (SSD); Implementing the SSD Consensus Protocol Into Clinical Routine. Otol Neurotol, 2020. 41(6): p. 727-735.
- Jakob, T.F., et al., Bone-anchored hearing system, contralateral routing of signals hearing aid or cochlear implant: what is best in single-sided deafness? Eur Arch Otorhinolaryngol, 2022. 279(1): p. 149-158.
- Potier, M., et al., Evaluation of a New Bone Conduction Device for the Rehabilitation of Single-Sided Deafness: Effects on Speech Understanding in Noise. Otol Neurotol, 2022. 43(1): p. 105-112.
- Sikka, K., et al., Objective Comparison of Benefits Derived From Contralateral Routing of Signal Hearing Aid and Bone Conduction Device in Noisy Surroundings in Patients With Single-Sided Deafness. J Audiol Otol, 2022. 26(4): p. 202-207.
- Bosman, A.J., et al., Bone-anchored hearing aids in unilateral inner ear deafness. Acta oto-laryngologica, 2003. 123(2): p. 258-260.
- Baguley, D.M., et al., The evidence base for the application of contralateral bone anchored hearing aids in acquired unilateral sensorineural hearing loss in adults. Clin Otolaryngol, 2006. 31(1): p. 6-14.
- Peters, J.P., et al., Review: Bone conduction devices and contralateral routing of sound systems in single‐sided deafness. The Laryngoscope, 2015. 125(1): p. 218-226.
- Arndt, S., et al., Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol Neurotol, 2011. 32(1): p. 39-47.
- Legris, E., et al., Cortical auditory responses according to hearing rehabilitation in unilateral hearing loss. Eur Ann Otorhinolaryngol Head Neck Dis, 2019. 136(6): p. 439-445.
- Oyamada, S., et al., Speech Perception in Noise and Sound Localization for Cochlear Implant With Single-Sided Deafness Compared With Contralateral Routing of Signal Hearing Aids. Otol Neurotol, 2023. 44(4): p. 331-338.
- Marx, M., et al., Cochlear Implantation and Other Treatments in Single-Sided Deafness and Asymmetric Hearing Loss: Results of a National Multicenter Study Including a Randomized Controlled Trial. Audiol Neurootol, 2021. 26(6): p. 414-424.
- Marx, M., et al., Treatment choice in single-sided deafness and asymmetric hearing loss. A prospective, multicentre cohort study on 155 patients. Clin Otolaryngol, 2021. 46(4): p. 736-743.
- Courtois, J. and J.H. Jensen, Cros Fitting of Hearing Aids Clinical and Experimental Results. Scandinavian Audiology, 1976. 5(3): p. 137-146.
- Williams, V.A., R.A. McArdle, and T.H. Chisolm, Subjective and objective outcomes from new BiCROS technology in a veteran sample. J Am Acad Audiol, 2012. 23(10): p. 789-806.
- Valente, M. and K. Oeding, Evaluation of a BICROS System with a Directional Microphone in the Receiver and Transmitter. J Am Acad Audiol, 2015. 26(10): p. 856-71.
- Oeding, K. and M. Valente, Sentence recognition in noise and perceived benefit of noise reduction on the receiver and transmitter sides of a BICROS hearing aid. J Am Acad Audiol, 2013. 24(10): p. 980-91.
- Kuk, F., et al., Effects of Training on the Use of a Manual Microphone Shutoff on a BiCROS Device. J Am Acad Audiol, 2015. 26(5): p. 478-493.
- Turton, L., et al., Guidelines for best practice in the audiological management of adults with severe and profound hearing loss. Seminars in Hearing, 2020. 41(03): p. 141-246.
- Desjardins, J.L., The effects of hearing aid directional microphone and noise reduction processing on listening effort in older adults with hearing loss. Journal of the American Academy of Audiology, 2016. 27(1): p. 29 - 41.
- Park, H., et al., Benefit From Directional Microphone Hearing Aids: Objective and Subjective Evaluations. Clinical and Experimental Otorhinolaryngology, 2015. 8(3): p. 237-242.
- Kim, J.S. and M.F. Bryan, The effects of asymmetric directional microphone fittings on acceptance of background noise. International Journal of Audiology, 2011. 50(5): p. 290-296.
- Cord, M.T., et al., Ear asymmetries and asymmetric directional microphone hearing aid fittings. American Journal of Audiology, 2011. 20(2): p. 111-22.
- Ricketts, T.A. and E.M. Picou, Symmetrical and asymmetrical directional benefits are present for talkers at the front and side. International Journal of Audiology, 2022. 61(3): p. 177-186.
- Hornsby, B. and T. Ricketts, Effects of noise source configuration on directional benefit using symmetric and asymmetric directional hearing aid fittings. Ear and Hearing, 2007. 28(2): p. 177-186.
- Kuk, F., et al., Performance of a fully adaptive directional microphone to signals presented from various azimuths. Journal of the American Academy of Audiology, 2005. 16(6): p. 333-347.
- Kuk, F. and D. Keenan, Efficacy of a reverse cardioid directional microphone. Journal of the American Academy of Audiology, 2012. 23(1): p. 64-73.
- Van de Heyning, P., et al., Towards a Unified Testing Framework for Single-Sided Deafness Studies: A Consensus Paper. Audiol Neurootol, 2016. 21(6): p. 391-398.
- Wu, Y.H. and R.A. Bentler, Impact of visual cues on directional benefit and preference: Part I-Laboratory tests. Ear and Hearing, 2010. 31(1): p. 22 - 34.
- Wu, Y.-H. and R.A. Bentler, The influence of audiovisual ceiling performance on the relationship between reverberation and directional benefit: Perception and prediction. Ear and Hearing, 2012. 33(5): p. 604-614.
- Grange, J.A. and J.F. Culling, The benefit of head orientation to speech intelligibility in noise. The Journal of the Acoustical Society of America, 2016. 139(2): p. 703-712.
- Grange, J.A., et al., Turn an ear to hear: How hearing-impaired listeners can exploit head orientation to enhance their speech intelligibility in noisy social settings. Trends in Hearing, 2018. 22: p. 2331216518802701.
- Spehar, B., S. Goebel, and N. Tye-Murray, Effects of Context Type on Lipreading and Listening Performance and Implications for Sentence Processing. J Speech Lang Hear Res, 2015. 58(3): p. 1093-102.